Advances in diagnosis and treatment of testicular cancer
BMJ 2022; 379 doi: https://doi.org/10.1136/bmj-2022-070499 (Published 28 November 2022) Cite this as: BMJ 2022;379:e070499
- 12nd Department of Oncology, Faculty of Medicine, Comenius University, National Cancer Institute, Bratislava, Slovakia
- 2Department of Pathology and Laboratory Medicine, Warren Alpert Medical School of Brown University, Lifespan Academic Medical Center, Providence, RI, USA
- Correspondence to M Chovanec michal.chovanec1{at}gmail.com
Abstract
Testicular cancer is a curable cancer. The success of physicians in curing the disease is underpinned by multidisciplinary advances. Cisplatin-based combination chemotherapy and the refinement of post-chemotherapy surgical procedures and diagnostic strategies have greatly improved long term survival in most patients. Despite such excellent outcomes, several controversial dilemmas exist in the approaches to clinical stage I disease, salvage chemotherapy, post-chemotherapy surgical procedures, and implementing innovative imaging studies. Relapse after salvage chemotherapy has a poor prognosis and the optimal treatment is not apparent. Recent research has provided insight into the molecular mechanisms underlying cisplatin resistance. Phase 2 studies with targeted agents have failed to show adequate efficacy; however, our understanding of cisplatin resistant disease is rapidly expanding. This review summarizes recent advances and discusses relevant issues in the biology and management of testicular cancer.
Introduction
Scientific developments in the field of testicular germ cell tumors (GCTs) have undergone a fascinating journey during the second half of the 20th century. Testicular cancer is the most common malignant tumor in young men with rising incidence worldwide.123 GCTs are now considered a curable cancer owing to the >95% cure rate in all patients and approximately 90% cure rate in patients with metastatic disease.45 Such excellent outcomes have never been achieved for any other solid tumor in modern oncology. In the past, most patients with metastatic disease had a poor prognosis; however, the implementation of cisplatin based chemotherapy regimens and the refinement of surgical procedures have led to a radical change in the prognosis of GCTs.67 Today, only approximately 5% of patients die from metastatic disease caused by cisplatin resistance.45 This review summarizes the most recent data regarding the diagnosis and management of testicular cancer and discusses recent developments in this field.
Sources and selection criteria
We searched the PubMed and Medline libraries between 1 February and 30 April, 2022 using keywords and keyword combinations: “testicular cancer, germ cell tumors, incidence, pathogenesis, imaging, PET/CT, stage I disease, advanced disease, metastatic disease, relapse, salvage chemotherapy, retroperitoneal lymph node dissection (RPLND), cisplatin resistant, machine learning, deep learning.” We also searched the relevant guidelines of the National Comprehensive Cancer Network (NCCN), European Society of Medical Oncology (ESMO), and European Association of Urology (EAU). Phase 3 randomized studies were prioritized when available. We included phase 1, phase 2, and retrospective studies, meta-analyses, and selected review articles. Reference lists in articles were also searched for additional relevant publications. We excluded case reports and literature published in languages other than English.
Shifting patterns in testicular cancer incidence
Testicular GCTs affect predominantly white men. The incidence of GCTs has been steadily rising during the past 30 years in characteristic regions. In 2020, the highest incidence was estimated in Scandinavian countries, western and central Europe (7-11 cases per 100 000), US and Canada (5-6 cases per 100 000), and Australia and Japan (7 and 4 cases per 100 000, respectively).89 Incidence has doubled in some countries of northern Europe over the past two decades.1011 In the US, the burden of GCT incidence is predicted to rise by 23.9% from 2020 to 2026.3 Rising incidence was historically pronounced in non-Hispanic white people. Rates among Hispanic people are now forecast to increase annually by 3.96%. Owing to this shift in incidence, the highest rate of GCTs in the US will be in the Hispanic population by 2026.2 European countries are expected to experience rising burdens of incidence between 2010 and 2035. However, incidence is expected to attenuate in high incidence countries such as Denmark, Norway, Switzerland, and Austria, and decline in Italy and Spain, while the largest increase is expected in Baltic and eastern European countries. The reasons for the change in the ethnical and geographical landscape of GCTs in the US and Europe are unknown. Expected trends in GCT incidence within the aging population are gradually lowering the burden; however, the opposite appears to be predicted for the next decade. One explanation for the decrease in incidence in high incidence countries could be the increased rate of immigration from low incidence countries. A study in Denmark showed that first generation immigrants have lower incidence rates of testicular cancer compared with second generation immigrants.12 This also appears to underline the influence of environmental factors. While the underlying cause for increased incidence in Hispanic men remains unknown, increased migration of Hispanic populations into the US also suggests the role of environmental factors.
Developmental origins of GCTs
The trigger point in the pathogenesis of GCTs is centered within primordial germ cells (PGCs), which are responsible for carrying heritable genetic information. PGCs undergo a malignant transformation in utero that leads to formation of germ cell neoplasia in situ (GCNIS), a precursor lesion of GCTs.1314 While the exact tumorigenic trigger leading to the developmental switch is unknown, several characteristics in the molecular landscape of this event have been described. Polyploidization and aneuploidization are the early key events for malignant transformation of PGCs.15 Polyploidy and aneuploidy with supernumerical X chromosomal gains are pathognomonic for GCTs, along with anomalies of the short arm of chromosome 12. Isochromosome 12p, which is a gain of the short arm of chromosome 12, has been historically recognized as a genomic hallmark found in most, but not all, GCTs.16 Single driver alteration does not seem to be responsible for the leading carcinogenic event. Driver mutations were discovered in the KIT, KRAS, and CDC27 genes in small cohorts of patients especially with seminoma. However, the evidence to support their role in all GCTs is insufficient.171819 Rather, a complex polygenic mechanism has been suggested, where a particular expression profile may be associated with an increased risk of GCTs.2021
Germ cell neoplasia in situ consists of cells resembling PGCs arrested before their first step of maturation into gonocytes. As such, these cells maintain totipotent properties allowing progression into seminoma or embryonal carcinoma. They characteristically express embryonic stem cell markers such as KIT, PLAP1, OCT4, NANOG, SOX17, LIN28, and several embryonic mRNAs and miRNAs,2223 but the drivers behind progression towards seminoma or embryonal carcinoma are unknown. However, when GCNIS expresses mostly SOX17 or SOX2, the anticipated emerging tumor will be a seminoma or embryonal carcinoma, respectively.2425 PGCs undergo erasure of genomic imprinting in their physiological stage, which is later re-established as a paternal imprint in premeiotic germ cells.26 This epigenetic reprogramming serves for gain of totipotent properties in PGCs. Upon polyploidization in this stage, further maturation is blocked and the cells undergo a transformation into GCNIS. Here, gain of 12p occurs accompanying progression into GCT.27 Development of overt cancer from GCNIS is associated with several possible differentiation pathways. Substantial epigenetic changes chaperone this transition and emerging histological subtypes of GCTs express distinct epigenetic signatures.27 The molecular landscape of seminomas is significantly different from non-seminomas in DNA methylation, mRNA, miRNA, and proteomic profiling.28 Seminomas manifest a completely unmethylated global DNA methylation pattern. Non-seminomas show a diverse methylation profile depending on the level of differentiation (fig 1).28
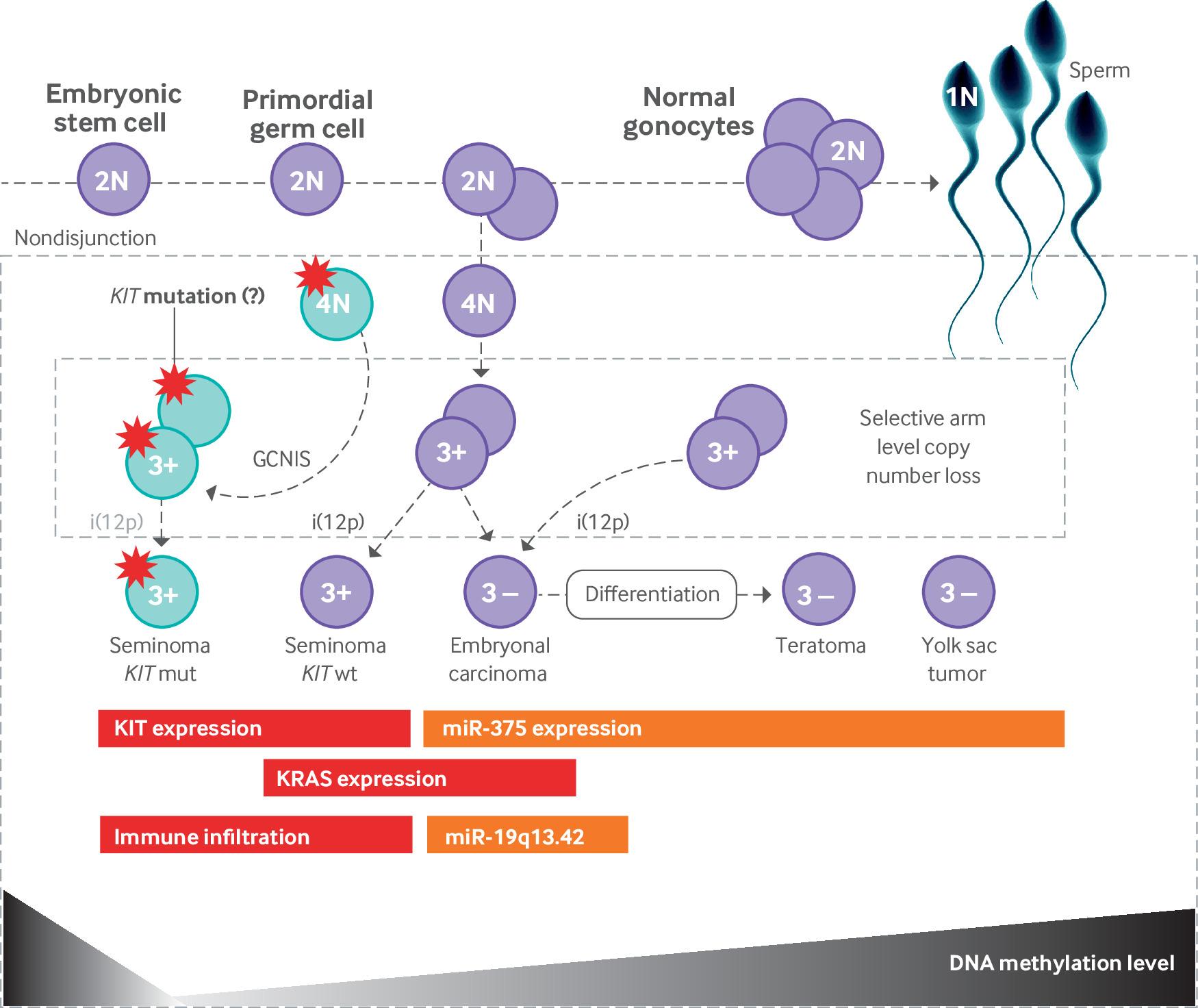
Molecular characteristics during pathogenesis of testicular germ cell tumors. 1-4N=cell ploidy (1-4 sets of chromosomes); GCNIS=germ cell neoplasia in situ; i(12p)=isochromosome 12p; KIT mut=KIT mutated; KIT wt=KIT wild type; miR=micro RNA. Modified from Shen H, Shih J, Hollern DP, et al. Integrated molecular characterization of testicular germ cell tumors. Cell Rep 2018;23:3392-406
{kind=link}
Diagnostic imaging in the era of modern oncology
Inguinal orchiectomy is an initial therapeutic procedure after finding a testicular tumor on physical examination and/or scrotal ultrasound. Standard diagnostic procedure requires measurement of pre- and post-orchiectomy serum tumor markers alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG) and performing an imaging study of chest, abdomen, and pelvis.
The role of positron emission tomography/computed tomography in the management of GCTs
The predictable pattern of metastatic spread in GCTs allows for reliable identification of metastatic lesions during the diagnostic investigation. After many attempts to refine imaging procedures with innovative methods, conventional computed tomography remains the standard in GCTs.29 Fluoro-deoxy glucose (FDG) positron emission tomography/computed tomography (PET/CT) scanning is often utilized in clinical practice. The use of this method for disease staging and management of GCTs is not supported by evidence.30 FDG PET/CT in stage I non-seminoma shows similar sensitivity and specificity to conventional computed tomography; however, the sensitivity to identify patients at risk of relapse is insufficient.3132 One multicenter diagnostic prospective study that evaluated patients with non-seminoma after orchiectomy was prematurely closed because of an excessively high relapse rate in PET/CT negative patients. In this study, 88 of 111 (79%) patients were PET/CT negative and all except one underwent surveillance. After 12 months of follow-up, 38% relapsed.32
One of the most important dilemmas in the multidisciplinary management of GCTs is an approach to residual disease after chemotherapy. The use of PET/CT when evaluating the post-chemotherapy retroperitoneal lymph nodes in non-seminoma has shown positive and negative predictive values of 91% and 62% and sensitivity and specificities of 59% and 92%, respectively.33 Post-chemotherapy residual lymph nodes larger than 1 cm may harbor viable cancer in 10-20%, and teratoma in 30-80% of cases (the percentage varies depending on whether there was teratoma in primary testicular tumor).343536 Teratoma, scar, and necrotic tissue have low uptakes of FDG during conventional positron emission tomography (PET) imaging (60 minutes after injection), which does not allow these tissue types to be distinguished.37 Unlike necrotic or scar tissue, teratoma tissue must be surgically resected to avoid the often fatal growing teratoma syndrome. Furthermore, relatively low negative predictive values and low sensitivities make detecting viable cancer difficult. Thus, the use of conventional PET/CT in the management of post-chemotherapy residual non-seminoma is not recommended. A small prospective diagnostic study in 21 patients showed that while not having the distinguishing standardized uptake values, measuring the kinetic rate constants of FDG uptake in these tissues could distinguish between teratoma, necrotic, and scar tissue. These constants were calculated to estimate the FDG transport from blood to tissue and an FDG phosphorylation rate within the tissue.37 Due to the small size of the study further validation on a larger population is essential.
Patients with pure seminoma and residual retroperitoneal mass represent a surgical challenge because of severe desmoplastic reaction surrounding the residual tissue. Surgical removal of these lymph nodes is often associated with extreme morbidity and may require multivisceral and multivascular resections. Such morbidity may be unnecessary in many patients. Studies performing FDG PET/CT in patients with seminoma after chemotherapy have shown positive and negative predictive values for lesions ≥3 cm of 23-50% and 94-96%, respectively.383940 While PET positive findings should be used with caution for further decision making, PET negative findings provide a strong argument for follow-up rather than surgery in this scenario.40 NCCN, ESMO, and EAU guidelines recommend using PET/CT only in patients with residual seminoma lesions >3 cm.3041 Lesions <3 cm in size almost never harbor a viable tumor4243; therefore, PET/CT does not provide much information on post-chemotherapy management and such patients should be closely monitored.
The role of magnetic resonance imaging
Magnetic resonance imaging (MRI) may be considered an alternative imaging method to conventional computed tomography. A prospective study in 52 patients showed non-inferiority of MRI to computed tomography with a reader sensitivity of 94% (95% CI 80 to 100) for MRI and 98% (95% CI 87 to 100) for computed tomography.44 However, MRI is generally not recommended for staging and monitoring of treatment effect.3044 Increased sensitivity and specificity were observed in a prospective diagnostic study using magnetic resonance with lymphotropic nanoparticles. Infused nanoparticles trapped in lymph nodes harboring metastases enhanced the sensitivity from 70.5% to 88.2% and specificity from 68% to 92% in a study performed in 18 GCT patients.45 A disadvantage of this approach is the necessity of two consecutive MRI scans 24 to 36 hours apart. Furthermore, these results have not been validated in larger prospective cohorts of patients.
Magnetic resonance imaging is the preferred method for the diagnosis of brain metastases according to current guidelines.293041 Brain metastases are found almost exclusively in patients with non-seminomas and are identified in 2-3% of patients with metastases.4647 Clinical suspicion for brain metastases should always be followed up by brain MRI imaging. There is no clear recommendation on whether to perform brain MRI in asymptomatic patients, but guidelines appropriately advocate for routine brain MRI in patients in the International Germ Cell Cancer Collaborative Group’s (IGCCCG) poor risk category.293041 Brain metastases may often have a hemorrhagic element, particularly the choriocarcinoma that often bleeds. Gradient echo susceptibility weighted imaging allows for detection of microhemorrhages via identification of degradation products of hemoglobin. This may be better than conventional MRI imaging for identifying occult metastases; however, confirmatory studies in GCTs are lacking.4849
Prognosis and biomarker evolution
Our ability to predict prognosis in GCTs has undergone substantial advancements in the past 30 years. A widely accepted risk stratification model for metastatic disease was introduced by the IGCCCG in 1997. Non-pulmonary visceral metastases, amplification of serum tumor markers AFP and HCG, and primary mediastinal non-seminoma were identified as determinants of poor prognosis. Based on these criteria, patients were stratified into good, intermediate, and poor risk categories with five year survival rates of 91%, 79%, and 48%, respectively.50 IGCCCG guidelines were updated in 2021 after effective international collaborations. Researchers worldwide merged their databases to bring together data on 12 179 patients with metastatic germ cell tumors.45 This work has led to improved outcomes in GCTs, when compared with the original IGCCCG classifications (tables 1 and 2).45 Five year overall survival in non-seminoma increased from 92% to 96% in the good risk group, from 80% to 89% in the intermediate risk group, and from 48% to 67% in the poor risk group.5 Five year overall survival in seminoma increased from 86% to 95% in good risk disease and from 72% to 88% in intermediate risk disease. Lactate dehydrogenase more than 2.5 times the upper limit of normal was an independent adverse prognostic factor in good risk disease.45 Further refinements were published introducing unfavorable (slower) marker decline after the first cycle of chemotherapy as a way of identifying patients with a 23% higher risk of death within the next two years.51 Based on this and other confirmatory studies, dose dense intensified chemotherapy was attempted in a phase 3 randomized study; however, it did not show an overall survival benefit.52 Unfavorable marker decline also proved to be prognostic in relapsed patients undergoing salvage chemotherapy.535455
Risk stratification of metastatic seminoma per the IGCCCG’s volume 2 guidelines*
Risk stratification of metastatic non-seminoma per the IGCCCG’s volume 2 guidelines*
Within the past two decades, several molecular biomarkers have been shown to have prognostic significance; one of them is miRNA371a-3p. This short, non-coding miRNA, involved in epigenetic regulation of gene expression, proved to be the most sensitive (>80%) and specific (>90%) in GCTs of all miRNAs that were investigated.565758 The level of miRNA371a-3p, which can be examined from peripheral blood, correlates with presence of all germ cell tumors except for teratoma and it seems to be associated with disease burden and prognosis5960; levels drop rapidly after orchiectomy for stage I disease.61 A validation study on 616 patients confirmed a sensitivity of 90.1%, specificity of 94%, and positive predictive value of 97.2%. In comparison, the positive predictive values for AFP, HCG, and LDH were ∼50%.62 Further studies have reported sensitivity, specificity, a positive predictive value, and a negative predictive value between 90% and 100%.6364 miRNA371a-3p shows great promise to become a reliable marker outperforming conventional serum markers and is expected to soon be implemented into clinical practice. The most likely scenarios for the use of miRNA371a-3p is in stage I disease and post-chemotherapy residual disease, to identify possible viable cancer not detectable by imaging.
Immune mechanisms seem to be involved in the pathogenesis and outcome of GCTs.65 Immune modulator program death ligand 1 (PD-L1) was shown to be a potent predictor of prognosis in patients with metastatic disease. Patients with low expression of PD-L1 on tumor cells had significantly longer progression free survival (PFS) (hazard ratio (HR)=0.40, 95% CI 0.16 to 1.01) and overall survival (HR=0.43, 95% CI 0.15 to 1.23).66 When expressed on tumor infiltrating lymphocytes (TIL), high expression of PD-L1 was associated with significantly longer PFS (HR=0.17, 95% CI 0.09 to 0.31) and overall survival (HR=0.08, 95% CI 0.04 to 0.16).67 Pro-inflammatory response evidenced by increased systemic immune inflammatory index (calculated as neutrophils/lymphocytes × platelets) and neutrophil to lymphocyte ratio are also highly potent predictors of poor prognosis in GCTs.6869 Furthermore, a prediction tool combining PD-L1 on TIL and stage II disease was able to identify patients who never progressed nor died of disease during 14 years of follow-up.68 While confident prognostic information may be gathered by examination of PD-L1 and inflammatory markers, anti-PD-1 and anti-PD-L1 agents did not prove effective in refractory patients in phase 2 trials.7071 Other biomarkers were shown to predict prognosis equally well. Higher concentrations of carbonic anhydrase 9, a marker of hypoxia, in the primary tumor was associated with poorer survival72 and β-1,4-galactosyltransferase-I in peripheral T lymphocytes identified patients with lower risk of relapse if treated with salvage high dose chemotherapy (HR=0.66, 95% CI 0.45 to 0.97).73 Patients with worse outcomes were also proven to have higher DNA damage in their peripheral blood mononuclear cells. The hazard ratio for overall survival was 14.62 (95% CI 3.14 to 67.95). More insights on predicting the rate of relapse in stage I seminoma came from a study assessing the expression DNA methyltransferase 3B (DNMT3B) in tissue samples. This study showed a significantly increased risk of relapse in patients with any DNMT3B expression compared with none.74
The exact implications of these preliminary molecular biomarker discoveries are not yet clear, although our understanding of the biology of GCTs has improved, which could lead to diagnostic and therapeutic advancements. However, guidelines do not recommend routine assessment of biomarkers except for AFP, HCG, and LDH.293041
Management of GCTs
Stage I disease
Approach to stage I disease has evolved substantially in the past decade. Stage I disease is characterized as tumor confined to the testicle, normal levels of serum tumor markers post-orchiectomy (half-life for AFP and HCG is 5-7 and 1-2 days, respectively), and a normal computed tomography scan. Patients with stage I disease present with very low risk of synchronous contralateral tumor/GCNIS. Routine contralateral testicular biopsy in all patients is not recommended by the guidelines, but may be used if there is a suspicion for contralateral tumor or risk factors are present (testicular volume <12 mL and/or history of cryptorchidism).293041 Accepted strategies in managing stage I testicular cancer are active surveillance or adjuvant chemotherapy with one cycle of carboplatin dosed at area under the curve (AUC) 7 for seminoma and active surveillance, adjuvant chemotherapy with one cycle of bleomycin, etoposide, cisplatin (BEP), or primary RPLND for non-seminoma.
Stage I seminoma
Orchiectomy alone will cure most patients with clinical stage I seminoma. About 10-20% of patients will experience disease relapse.757677 Several independent risk factors for estimating relapse rate have been researched. Tumor size and infiltration of rete testis are the most consistently reported.757677 A pooled analysis of four surveillance studies reported higher risk of relapse in patients with tumors >4 cm in size and rete testis invasion. Five year risk of relapse was 15.9% and 31.5% if one or two risk factors were present, respectively.7577 Tumors without risk factors yielded a five-year relapse rate of 4%.78 When researchers attempted to validate these risk factors, the results did not provide sufficient evidence to support the routine use of this prediction model in stage I seminoma.7980
The risk of relapse may be reduced with adjuvant treatment. Adjuvant radiotherapy of 20 gray units to the retroperitoneal lymph nodes results in relapse rates between 0.5% and 5%.818283 The use of adjuvant radiotherapy carries a significant risk of developing second cancers. Twofold to sixfold risk of second cancers after radiotherapy was reported from large population based cohorts after 10-16 years of follow-up.848586 Because of this significant risk of life threatening late toxicity, adjuvant radiotherapy is no longer recommended for the management of stage I seminoma except in exceptional cases.293087 Another option is administration of a single cycle of adjuvant carboplatin dosed at AUC7. Studies assessing the efficacy of adjuvant carboplatin found that the risk of relapse after one cycle is 2-9%, depending on the presence of risk factors.888990 Two cycles of adjuvant carboplatin previously given in the adjuvant setting were proven to be unnecessary. A randomized study in 1477 patients suggested that one cycle of carboplatin is acceptable (five-year relapse free rates of 94.7% and 96% for one versus two cycles).89
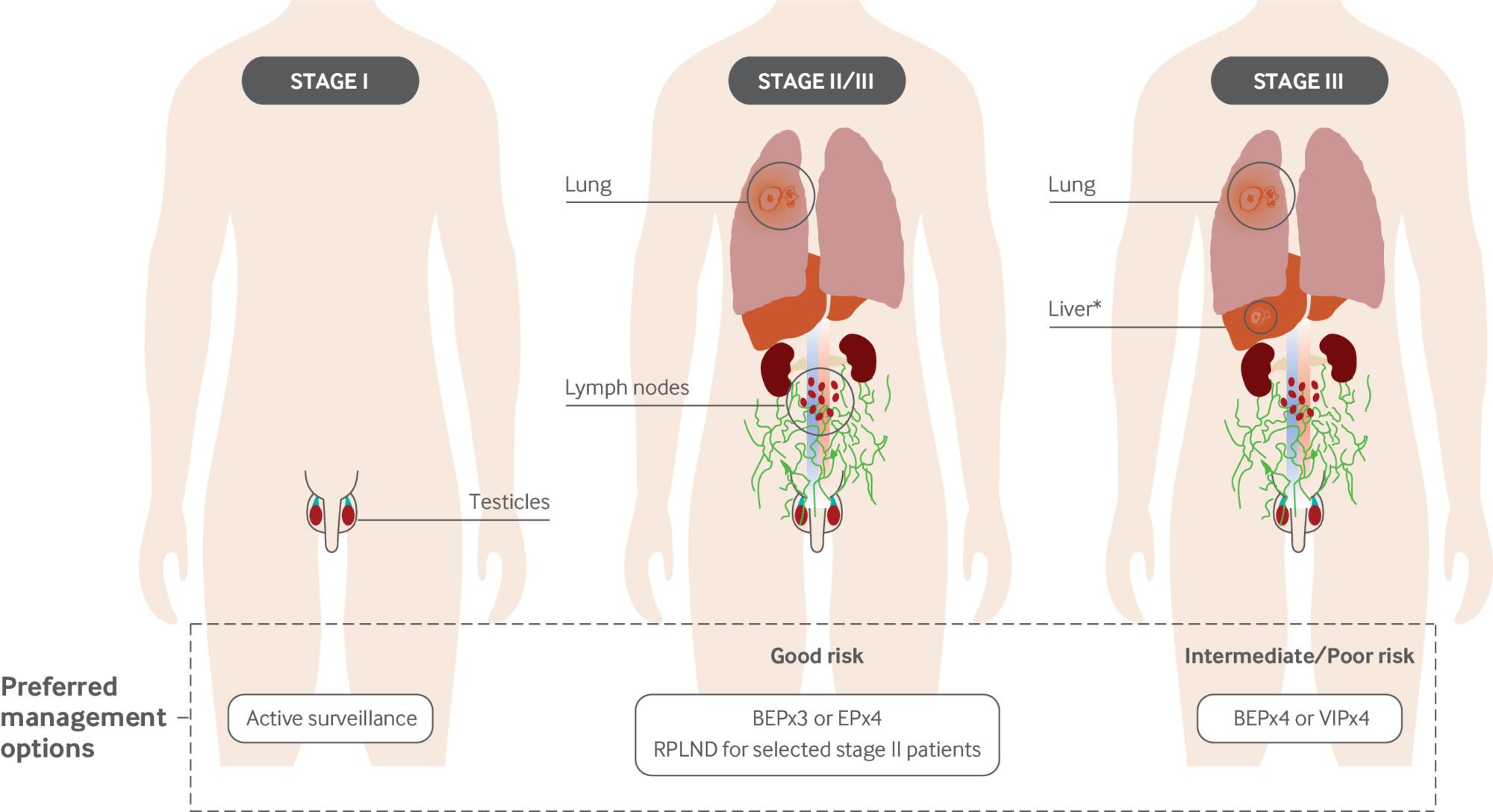
The option preferred by most international expert institutions and guidelines is active surveillance (fig 2).294187 The advantage in managing GCTs compared with other solid tumors is their unique sensitivity to cisplatin. If surveilled appropriately, patients relapsing from stage I seminoma are cured in 99-100% of cases. Therefore, the general approach is to spare the majority patients of unnecessary toxicity while treating relapsed patients with systemic chemotherapy.91

Preferred management options in testicular cancer. Active surveillance is the preferred management in all clinical stage I disease patients. An alternative is one cycle of adjuvant carboplatin AUC7 for stage I seminoma and adjuvant BEP × 1 or RPLND for non-seminoma. Stage II disease is primarily managed with BEP × 3 or EP × 4; however, marker negative non-seminomas and seminomas with lymph nodes <3 cm may be treated with RPLND. Good risk disease is managed with BEP × 3 or EP × 4. Intermediate risk disease is characterized by absence of non-pulmonary visceral metastases, but serum tumor markers are in the SII stage (AFP 1000-10 000 ng/mL and HCG 5000-50 000 mIU/mL). Intermediate/poor risk disease is managed with BEP × 4 or VIP × 4. VIP is used when bleomycin is contraindicated (history of heavy smoking, renal impairment, or aged >50), extensive lung metastases are present, and when extensive pulmonary surgery after chemotherapy is anticipated. *Poor risk disease includes patients with any non-pulmonary visceral metastases. AUC7=area under the curve 7; BEP=bleomycin, etoposide, cisplatin; EP=etoposide, cisplatin; RPLND=retroperitoneal lymph node dissection; VIP=etoposide, ifosfamide, cisplatin
{kind=link}
Stage I non-seminoma
Stage I non-seminoma may consist of a single histological subtype such as embryonal carcinoma, yolk sac tumor, choriocarcinoma, teratoma, or mixed tumor with any subtype including seminoma. Widely accepted risk factors are a predominance of embryonal carcinoma during pathological evaluation and a presence of lymphovascular invasion (LVI).9293 A large meta-analysis showed presence of occult metastases in 47.5% and 16.9% in LVI positive and LVI negative patients, respectively. Pooled rates of occult metastases were 33.2% for embryonal carcinoma presence and 16.2% for embryonal carcinoma absence.94 The relevance of presence/predominance of embryonal carcinoma is discussed, as different studies used different criteria for definition.
Stage I non-seminoma is cured with orchiectomy alone in 50-80% of patients. Management strategies for clinical stage I non-seminoma include active surveillance, one cycle of BEP, or primary RPLND. Adjuvant chemotherapy with BEP × 1 will lower the risk of relapse to 0-6.5% regardless of LVI according to studies.9596979899100101 Patients who are subjected to primary RPLND will relapse in 8-18% of cases.102103 RPLND may result in retrograde ejaculation; therefore, these surgeries should be performed only in high volume centers by experienced surgeons who can salvage antegrade ejaculation with nerve-spring techniques in more than 99% of patients.104 Despite higher relapse rates in clinical stage I non-seminoma, the relapses are almost exclusively in the IGCCCG’s good risk group and the cure rates remain between 99% and 100%.91 Both seminomas and non-seminomas in clinical stage I have unchanged overall survival regardless of treatment approach. The argument arises as to whether to overtreat most patients with unnecessary adjuvant treatment, or whether to treat relapses with 3-4 cycles of chemotherapy with cure rates of 99-100%.91 Based on this argument, most experts and relevant guidelines advocate for active surveillance in all stage I testicular GCTs to spare many patients unnecessary toxicities; however, adjuvant treatment is acceptable especially in high-risk patients.294191
Five year active surveillance protocols have been substantially de-intensified since the 1980s. Computed tomography scanning was reduced to 5-10 scans of the abdomen with or without the pelvis (computed tomography of the pelvis is added when the patient has a history of scrotal surgery, vasectomy, inguinal hernia, or undescended testicle) and the number of chest x ray images decreased from up to 30 to between 0 and 10. Some institutions utilize low dose computed tomography for chest scanning.91105 Even though the surveillance protocols are less intensive nowadays, no difference in relapse burden has been observed in terms of lymph nodes, visceral metastases, serum tumor markers, or IGCCCG risk group. A case series of 1583 patients surveilled in Canada found that the death rate remained unchanged from 1981 to 2020.105
If rising tumor markers occur after orchiectomy without evidence of metastases on imaging (stage I), patients should undergo systemic chemotherapy.29
Stage II seminoma
Stage II disease includes patients with metastatic spread into retroperitoneal lymph nodes. The approach to management of stage II seminoma has changed during recent years. Historically, patients with lower volume stage II disease (stage IIA and stage IIB) underwent curative radiotherapy to the retroperitoneum and ipsilateral pelvic lymph nodes, which was later reduced to the retroperitoneum only.106107108 Radiotherapy presents a substantially increased risk of second cancers. About 10-30% of patients will relapse after radiotherapy and require salvage chemotherapy.109 In patients who have received one course of radiotherapy and chemotherapy during their lifetime, the risk of dying from a non-testicular cancer cause and second cancers is 2.04-fold and 3.24-fold compared with the general population, respectively.86110 Many experts therefore avoid radiotherapy in stage II seminoma. An accepted option is to give three cycles of BEP or four cycles of etoposide, cisplatin (EP) which proved to have similar relapse rates and similar overall survival. A retrospective study in 67 patients treated with chemotherapy for stage IIA-C seminoma reported a five year overall survival of 97% (95% CI 89 to 99).109 Another retrospective study treating patients with stage IIA-B seminoma with chemotherapy has shown a 95% overall survival (95% CI 89 to 100). Patients with lymph nodes <2 cm (stage IIA), who had been most commonly referred to radiotherapy in the past, had a five year PFS of 100% with chemotherapy.111 These results support the rationale for avoiding radiotherapy in the setting of stage II seminoma.
Surgical treatment with RPLND has been also proposed as a treatment option to spare patients the toxicity of chemotherapy or radiotherapy. A multi-institutional phase II trial from the US included 55 patients with stage II seminoma and retroperitoneal lymphadenopathy 1-3 cm in size. Recurrence rate was 18%, all relapsing patients were salvaged with chemotherapy with a five year overall survival of 100%, and none of the patients reported long term complications from surgery.112 The German single-arm PRIMETEST study has shown a 69% recurrence free rate in stage IIA-B patients treated with RPLND at 26 months of follow-up. However, 58% of procedures were carried out robotically.113 Retroperitoneal lymph node dissection may be an important step in shifting the management of stage II seminoma as 70-80% of patients could be spared the toxicity of chemotherapy (fig 2). Another multicenter single arm phase II study used sequential single dose carboplatin followed by involved node radiotherapy in 120 stage IIA-B seminomas and showed a 92.6% and 95.2% three year PFS, respectively. Seven patients (5.8%) relapsed and there were four (3.3%) second primary cancers including two seminomas, renal cancer, and cholangiocarcinoma.114
Stage II non-seminoma
Stage II non-seminoma is mostly managed with chemotherapy with BEP × 3 or EP × 4. Patients with serum markers in the normal range and lower volume retroperitoneal lymph nodes (<3 cm) may undergo nerve sparing RPLND.29115 The argument to utilize RPLND instead of chemotherapy stems from an effort to spare patients unnecessary chemotherapy. The cure rate with up-front RPLND is 95-99% and allows for accurate pathological staging.115116 Multifocal disease, rising markers, and lymph nodes larger than 3 cm should be treated with chemotherapy. Patient selection for chemotherapy versus RPLND must be done cautiously. A retrospective series of 252 patients reported that appropriate selection of patients improved relapse free rate in patients undergoing RPLND for stage II disease from 78% to 100%.117
Stage III disease
Patients with metastases beyond the retroperitoneum are categorized as having stage III disease. Good risk disease per IGCCCG criteria includes patients who may have metastases in distant lymph nodes and/or lungs and/or serum tumor markers remain in the stage I range (<5000 IU/L for HCG and <1000 ng/mL for AFP) (tables 1 and 2). The exception is pure seminoma, which lacks the poor risk category (table 1) and does not show a significant elevation of AFP and HCG.5 The discovery of cisplatin by Rosenberg in 1965 and its implementation into combined cytostatic regimen by Einhorn in 1974 led to a revolutionary change in the prognosis of metastatic GCTs.6118 Subsequent trials have refined and substituted the original cisplatin, vinblastine, bleomycin (PVB) regimen for BEP.119 Four cycles of BEP were later abbreviated to three cycles, as phase III randomized studies have shown identical outcomes with significantly less toxicity in patients then characterized as low risk.120121 A regimen omitting bleomycin from the treatment was simultaneously developed to spare patients the pulmonary toxicity of bleomycin.122 EP × 4 was later shown to be non-inferior to BEP × 3 in a phase III randomized trial with 92% and 96% four year overall survival rates, respectively (HR=0.42, 95% CI 0.15 to 1.20).123 Currently, BEP × 3 or EP × 4 remains the standard of care for good risk patients.293041
Chemotherapy regimens for intermediate risk patients (those with SII tumor markers, eg, HCG 5000-50 000 IU/L or AFP 1000-10 000 ng/mL) and poor risk patients (those with non-pulmonary visceral metastases or HCG >50 000 IU/Lor AFP > 10 000 ng/mL) include BEP × 4 or etoposide, ifosfamide, cisplatin (VIP) × 4 in select patients who cannot receive bleomycin (fig 2). Intermediate risk patients achieve a cure rate of 88-89% in contemporary cohorts.45 Researchers have attempted to improve the 50-60% cure rates in poor risk patients by conducting numerous trials with intensified chemotherapy schedules during the past 20 years. Some have tried adding paclitaxel to BEP124125126; others have used various high dose chemotherapy regimens with stem cell support127128129130131 or risk stratification to complicated dose dense regimens based on unfavorable marker decline after the first cycle of chemotherapy.132 Unfortunately, none of these studies have shown benefit on overall survival and, because of their complicated nature and increased toxicity, were never adopted in clinical practice.
Salvage treatment
Despite unique sensitivity to cisplatin based chemotherapy, 20-30% of patients relapse after first line treatment.133134135136 These patients require salvage chemotherapy. Very select patients may be candidates for salvage surgery if the relapse is confined to one anatomical site, such as retroperitoneum. This approach can cure about 20% of relapsed patients. A study evaluated salvage/desperation surgery in anatomically confined relapses within their original site of appearance. Of 48 patients, 21% remained disease free after surgery only without the need of subsequent chemotherapy.137 Most of the relapsed patients are, however, candidates for salvage chemotherapy with cure rates of 20-60%.137 The outcome is dependent on selected chemotherapy regimens, timing of relapse, performance status, and disease biological landscape.134138139 Two accepted approaches have been developed in the salvage setting: conventional dose chemotherapy (CDCT) and high dose chemotherapy (HDCT). Treatment with CDCT requires previously unused agents, such as paclitaxel, ifosfamide, cisplatin (TIP), VIP, or the older regimen vinblastine, ifosfamide, cisplatin (VeIP). Patients are cured in 20-40% of cases with CDCT.136140141 Several studies were conducted in recent decades to answer the question of whether higher doses of chemotherapy can overcome resistance to CDCT. Relapsed GCT is a rare and challenging population in which to conduct high quality phase 3 randomized trials. Two randomized phase 3 studies have been conducted. The first study compared four cycles of CDCT (VIP or VeIP) with three cycles of CDCT and one cycle of HDCT with carboplatin, etoposide, and cyclophosphamide. There was no overall survival benefit (53%, 95% CI 46 to 59%).142 The second study compared one cycle of CDCT and three cycles of HDCT with etoposide and carboplatin versus three cycles of CDCT and one cycle of HDCT with etoposide, carboplatin, and cyclophosphamide. This study was prematurely closed because of excess deaths in the second arm and no overall survival benefit of the experimental approach.143 Reported randomized studies have several limitations such as selection bias and flaws in design. A phase 1/2 trial from Memorial Sloan Kettering Cancer Center and two large retrospective studies from Indiana University have consistently shown 50-60% durable cure rates using two cycles of HDCT with etoposide and carboplatin (Indiana regimen) or three cycles of conventional dose paclitaxel and ifosfamide followed by HDCT carboplatin, etoposide (Memorial regimen; TI-CE). A retrospective study comparing HDCT and CDCT in 821 and 773 patients treated in 38 centers worldwide have shown an overall survival benefit in very low, intermediate, high and very high risk patients (HR range 0.24-0.62), but not in low risk patients (HR=1.00, 95% CI 0.62 to 1.63).144 Autologous stem cell rescue is an essential supportive treatment after HDCT.138139145 A recent retrospective study from Indiana University reported on three 28 day cycles of maintenance chemotherapy with daily oral etoposide after HDCT in non-seminoma patients. Patients receiving maintenance therapy had longer PFS (55% v 44%, P=0.008) and overall survival (61% v 52%, P=0.01).146
Using HDCT over CDCT presents an ongoing dilemma. Some centers advocate for HDCT in all relapsed patients while others argue that some patients are overtreated with this approach. Guidelines suggest both CDCT and HDCT as a preferred option for salvage treatment.293041 Currently, there is no reliable prognostic model to safely select patients for HDCT. Patients may be salvageable in the third or subsequent lines of therapies; however, the toxicity is much higher and cure rates decline.138 This controversial question may be closer to being resolved with an ongoing phase 3 randomized study (NCT04804007) comparing TIP × 4 with TI-CE × 3.147 Further relapses after salvage chemotherapy are considered incurable. Limited efficacy and very rare cures may be seen with regimens such as gemcitabine, oxaliplatin with or without paclitaxel, or epirubicin and cisplatin.148149
Post-chemotherapy surgery
Post-chemotherapy surgical techniques are a necessary component of multidisciplinary care in GCTs. If residual metastatic sites were identified after the final course of chemotherapy (initial or salvage), all lesions should be surgically removed.150151152153 The most common site of residual disease is the retroperitoneum. Post-chemotherapy retroperitoneal lymph node dissection (PC-RPLND) is required in non-seminoma with residual lymph nodes larger than 1 cm in the absence of elevated serum tumor markers.2941 There is disagreement among experts as to whether to also surgically remove lymph nodes <1 cm because of occasional presence of active cancer (4%) and teratoma (24%).154 A meta-analysis evaluating outcomes in patients with sub-centimeter residual lymph nodes found only 3% of relapses in the retroperitoneum without surgery. Two of 15 patients who relapsed in the retroperitoneum eventually died from GCT.155 In monitoring patients who achieved a complete response with retroperitoneal lymph nodes < 1 cm, 97% of patients undergoing surveillance with no further treatment achieved 15 year overall survival.156 Subjecting all patients with sub-centimeter residual lymph nodes to PC-RPLND would lead to overtreatment in most patients. On the other hand, patients with lymph nodes >1 cm were found to have teratoma in 30-80%, and viable GCT in 10-15% of cases in the histological specimen.343536150 PC-RPLND techniques have evolved substantially since the 1960s. Unilateral template surgery entailing the landing zone of primary tumor may be safely performed if the post-chemotherapy size of lymph nodes does not exceed 5 cm. This approach maintains ejaculatory function in 87% of patients compared with 44% of those undergoing bilateral template resection.157 Bilateral template resection is needed in patients with retroperitoneal masses larger than 5 cm or located bilaterally. The one and two year survival rates with unilateral versus bilateral template were 91% and 91%, and 77% and 72%, respectively (P=0.0078).157
Surgical treatment of residual seminoma presents a challenge. As mentioned above, viable cancer is almost never present in residual retroperitoneal disease <3 cm4243 and these patients should be monitored. Residual masses >3 cm that are PET/CT negative have ∼5% chance of having viable tumor and are generally not recommended for PC-RPLND.383940 Surgeries in chemotherapy pretreated seminomas are extremely difficult because of desmoplastic reaction surrounding the tissue. PET/CT positive retroperitoneal lymph nodes >3 cm present one of the most challenging decision dilemmas. Our recommendation is to offer these patients PC-RPLND if the urology surgeon considers the risk of morbidity low. If the morbidity is not acceptable, we suggest observation and salvage chemotherapy upon relapse. This recommendation is based on our clinical experience rather than clear evidence. Data to guide management in this rare scenario are limited and guidelines do not address this specific issue. Salvage chemotherapy at presence of growing mass is recommended by EAU guidelines.41
In recent years there have been initiatives to decrease the morbidity of surgery with minimally invasive surgery. Studies performing laparoscopic and robotic assisted surgeries report satisfactory therapeutic results and low to no morbidity.158159160161162 However, a study assessing patients referred to Indiana University for recurrence reported aberrant recurrence patterns after minimally invasive surgeries. All five patients had recurrences in abnormal locations compared with past routine experience. One patient had in-field recurrence close to the lumbar vessels and four patients had out-of-field recurrence in the pericolic space invading the colon, peritoneal carcinomatosis, extensive liver metastases with supra-hilar lymph nodes, and celiac lymph nodes. Minimally invasive surgery is not recommended by guidelines and should therefore remain an experimental approach.293041
Underpinnings of cisplatin resistance and biomarker driven clinical trials
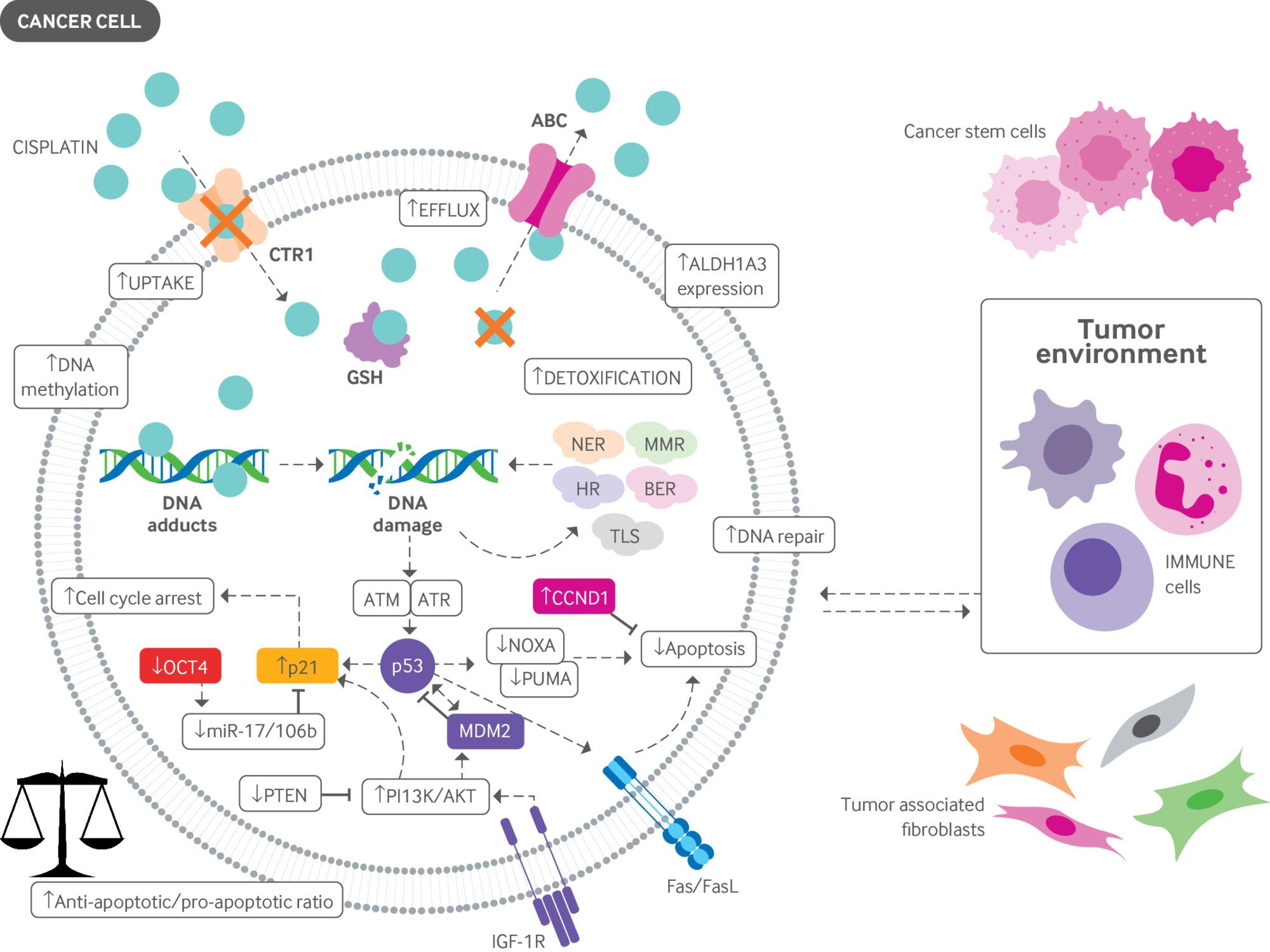
Overcoming cisplatin resistance is the most important scientific and clinical challenge in GCTs. Several mechanisms have been proposed and investigated (fig 3). Pre-target mechanisms lead to decreased accumulation of cisplatin in the cell (by reduced uptake or increased efflux) and increased detoxification in cytoplasm.163 Downregulated transmembrane transporter for cisplatin (CTR1) and upregulated efflux mediating ATPases ATP7A and ATP7B were identified as responsible for lowering the intracellular cisplatin concentrations in cell line experiments.164165166 On-target mechanisms include DNA repair pathways that are normally of low activity in GCTs. The nucleotide excision repair (NER) pathway seems to be activated in cisplatin-resistant GCT cell lines and upregulation of proteins involved in the NER pathway correlate with poor patient outcome.167168 PARP, an enzyme involved in base excision repair was found to be overexpressed in GCTs with a trend to poorer overall survival in patients with higher PARP expression.169 Microsatellite instability and BRAF mutations were also found to be present in cisplatin resistant tumors170 and mismatch repair genes MLH1 and MLH2 were upregulated in cisplatin resistant cell lines.171 Post-target mechanisms lead to downregulation of p53, the resulting inhibition of tumor suppressor pathways, and the dysregulation of the PDGFR/PI3K/AKT pathway with extensive expression of its regulator PTEN.172 Furthermore, overexpression of pluripotency markers such as the 1A3 isoform of aldehyde dehydrogenase was identified in resistant GCT cell lines.173 Epigenetic changes may also play a contributing role, as tumors showing a hypermethylated pattern were found in cisplatin resistant cell lines and patient specimens.174 Cisplatin resistance is also associated with aberrant regulation of the WNT/βcatenin pathway, which leads to an increase in pluripotency and the immune-suppressive microenvironment.175176 The pro-inflammatory microenvironment may further allow for tumor escape from the cytostatic effect. Distinct immune phenotypes and cytokine profiles can be found in patients with advanced disease stages where pro-tumorigenous cell populations and pro-inflammatory signaling can be identified.177178 Several attempts to overcome cisplatin resistance in clinical trials have failed; however, sustained efforts to continue this initiative are imperative.

Mechanisms of resistance to cisplatin. Pre-target mechanisms allow for decreased accumulation of cisplatin in cancer cells via reduced uptake or increased efflux. On-target mechanisms include increased DNA repair capabilities or increased DNA damage tolerance. Post-target mechanisms include altered apoptotic pathways leading to cell cycle arrest and inhibition of apoptosis. Epigenetic alterations, increased expression of stem cell markers, and the immune microenvironment are further contributors to cisplatin resistance. ABC=ATP-binding cassette transporter; AKT=protein kinase B (PKB); ALDH1A3=aldehyde dehydrogenase 1A3; ATM=ataxia telangiectasia mutated; ATR=ATM and RAD3-related; BER=base excision repair; CCND1=cyclin D1; CTR1=copper transporter protein; FasL=Fas ligand; GSH=glutathione; HR=homologous recombination; IGF-1R=insulin-like growth factor 1 receptor; miR-17/106b=microRNA-17/106b; MDM2=mouse double minute 2 homolog; MMR=mismatch repair; NER=nucleotide excision repair; NOXA=Phorbol-12-myristate-13-acetate-induced protein 1; OCT-4=octamer binding transcription factor 4; PI3K=phosphoinositide 3-kinase; PTEN=phosphatase and tensin homolog; PUMA=p53 upregulated modulator of apoptosis; TLS=translesion synthesis. Modified from Országhová Z, Kalavska K, Mego M, et al. Overcoming chemotherapy resistance in germ cell tumors. Biomedicines 2022;10:972
{kind=link}
Guidelines
The most relevant guidelines on the management of GCTs have been developed by the NCCN, ESMO, and EAU.293041 The NCCN guidelines were last updated in 2020. While they provide a thorough and comprehensive guide to GCT management, the focus is on non-seminoma. Guidelines on the management of seminoma in specific scenarios such as stage I-III disease and post-chemotherapy surgery are lacking. We consider this to be a great weakness of otherwise very thorough guidelines. The ESMO guidelines provide consistent recommendations on diagnosis and management in all stages of GCTs including important recommendations on long term follow-up and survivorship care. An ESMO consensus conference on testicular cancer held in 2018 addressed many of the unanswered questions.87 The EAU guidelines were last updated in March 2022, providing the most up to date recommendations. These guidelines are very comprehensive in all aspects of testicular cancer management including late toxicities of treatments.
All guidelines are consistent on fundamental aspects of GCT management. Approach to stage I disease is to favor surveillance and offer adjuvant treatment as an option after discussion with the patient. Recommendations in high-risk stage I non-seminoma (LVI+) are surveillance or adjuvant BEP × 1 as equal options.293087 The 99-100% cure rates in cases of relapse under surveillance allow for this “surveillance for all” approach to spare patients the unnecessary toxicity of adjuvant treatment if the patient consents to the surveillance protocol. Recommendations of guidelines on management of metastatic disease agree on using BEP × 3 or EP × 4 for good risk disease and BEP × 4 or VIP × 4 for intermediate and poor risk disease.293041 BEP × 3 or EP × 4 have proven to provide similar overall survival in phase 3 randomized trials; however, the use of one over another differs according to the routines in different expert centers.123 Recommendations on salvage chemotherapy are consistent in that CDCT (TIP, VeIP, or VIP) or HDCT should be used as equal options.293041 HDCT seems to provide superior results based on retrospective data; however, the level of evidence in the absence of phase 3 randomized trials is insufficient to support a recommendation. On the other hand, the use of CDCT regimens recommended by guidelines in the salvage setting is also not supported by phase 3 randomized trials because these were never conducted. We believe that in the absence of phase 3 randomized trials, regimens showing exceptional activity in phase 2 trials or retrospective studies are appropriately recommended by available guidelines.293041
Emerging treatments
A single arm phase 2 study with a potent MET inhibitor cabozantinib is currently ongoing and the results are expected in December 2025 (NCT04876456). The anti-CD30 agent brentuximab-vedotin showed one complete response (CR) and one partial response (PR) in nine patients.179 One promising study demonstrated two CRs and three PRs with the demethylating agent guadecitabin plus cisplatin in 14 patients with refractory disease.180 Beside the translational research driven studies, there are ongoing efforts to refine the treatment in specific scenarios. The SWENOTECA-ABC trial assesses BEP × 1 as an adjuvant treatment for stage I seminoma with risk factors and the expected date of reporting is December 2035 (NCT02341989). The SAKK 01/18 trial (NCT03937843) aims to use a sequential single cycle of carboplatin with subsequent involved-node radiotherapy in stage II seminomas to substitute for three to four cycles of cisplatin based chemotherapy. The ongoing SEMITEP trial (NCT01887340) is attempting to de-escalate treatment intensity in good risk metastatic seminomas based on the result of PET/CT after two cycles of chemotherapy. One of the most important studies, which is expected to be reported in June 2024, is the “Tiger” phase 3 randomized study that compares standard dose salvage regimen TIP × 4 and HDCT with TI-CE × 3 (NCT02375204). A maintenance oral etoposide after HDCT is currently being investigated in a randomized phase 2 trial, with results expected in December 2026.
Beyond conventional medicine
Artificial intelligence (AI) has emerged in contemporary medicine much like it has in other fields of research and technology. One recent retrospective radiomics study used machine learning (a computer uses algorithms without specific training) to create a predictive model for small testicular lesions based on T2 weighted MRI imaging. Testicular MRI scans of 42 patients were retrospectively assessed by two radiologists who segmented the volume of interest. Subsequently, a computer was allowed to train using linear model and linear support vector machine algorithms to assess the discrimination between GCT versus non-GCT and seminoma versus non-seminoma. Acquired accuracy was 89% and 86%, respectively.181 A retrospective study using deep learning technology (using complex algorithms modeled on the human brain) attempted to detect TILs within GCT tissue. Researchers obtained a correlation coefficient of 0.89 when comparing the manual count with the computer algorithm. Interobserver agreement between the algorithm and experts and between experts themselves was higher for the former (kappa=0.35 v 0.32, indicating fair agreement).182 Machine learning was also used to try to predict the histology in PC-RPLND in a retrospective radiomics study that included histological samples from 80 patients. Trained machines were able to identify benign (necrosis/fibrosis) and malignant (viable cancer/teratoma) tissue with 88% specificity, 72% sensitivity, and 88% negative predictive value.183 Identifying teratoma and active cancer in post-chemotherapy residual mass is one of the most difficult tasks in the clinical management of GCTs; therefore, this investigation is helping to plug a frustrating knowledge gap. Investigators from Denmark used machine learning algorithms to predict nephrotoxicity induced by cisplatin based on genomic markers found in DNA obtained from saliva. Genomic markers associated with nephrotoxicity were found at NAT1, NAT2, and the intergenic region between CNTN6 and CNTN4. These, combined with previously found markers located at ERCC1, ERCC2, and SLC22A2 and clinical characteristics, led to a receiver operating characteristic curve of 0.731 (95% CI 0.726 to 0.736).
With future validation, AI shows great promise in becoming a powerful tool to improve diagnosis and treatment outcomes. Further investigations are required for validation and implementation into clinical practice.
Conclusion
GCTs represent a unique cancer in terms of their biology, diagnosis, and achievable cure. Many advances in the understanding of the molecular basis of pathogenesis and cisplatin resistance, the refining surgical procedures, and the search for innovative biomarkers and diagnostic tools have been recently made. Unfortunately, our current knowledge is still insufficient to overcome the poor prognosis of patients who do not respond to salvage chemotherapy. However, our growing understanding of testicular cancer is building a basis for ultimately finding a cure for all patients. Modern molecular biology methods have allowed for important discoveries in the field of biomarkers. The emerging field of artificial intelligence may help to process the vast amounts of data acquired during research. In the absence of new effective drugs, the new IGCCCG classification volume 2 suggests that the growing expertise in treating GCTs has been of critical importance to the improved survival rates seen within the past 30 years. Such expertise should be carefully honed to further improve outcomes for our patients.
Questions for future research
What is the optimal implementation of miRNA 371a-3p into clinical practice?
In post-chemotherapy residual disease, can we achieve high precision in predicting the histology to spare patients complicated surgical procedures?
Is salvage high dose chemotherapy superior to conventional dose chemotherapy in relapsed patients?
In refractory disease, what are the missing key targetable drivers of cisplatin resistance?
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Contributors: MC and LC contributed equally to the manuscript idea, literature search, and review article writing. LC is the guarantor.
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Funding: Slovak Research and Development Agency under contract no. APVV-15-0086 and APVV-19-0411 and VEGA 1/0327/19 for MC.
Patient involvement: no patients were involved.
Provenance and peer review: Commissioned; externally peer reviewed.