Association of China’s universal two child policy with changes in births and birth related health factors: national, descriptive comparative study
BMJ 2019; 366 doi: https://doi.org/10.1136/bmj.l4680 (Published 21 August 2019) Cite this as: BMJ 2019;366:l4680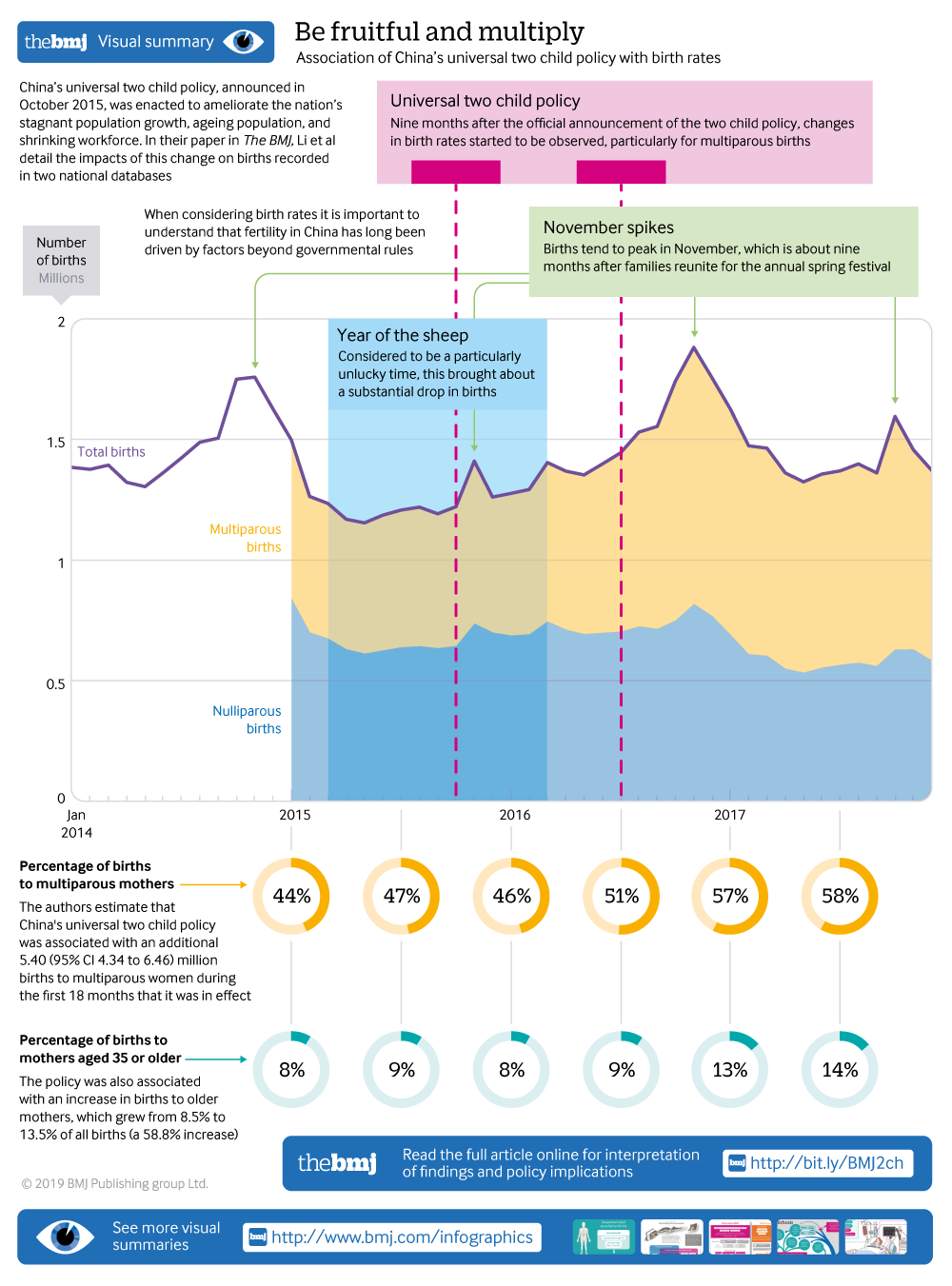
Visual summary available
Explaining trends in birth rates following introduction of China's universal two child policy
Linked opinion
Jian-Meng Liu: The cast of thousands behind our data

- Hong-tian Li, associate professor1 2 3,
- Ming Xue, senior statistician4,
- Susan Hellerstein, assistant professor5,
- Yue Cai, associate professor4,
- Yanqiu Gao, lecturer2 6,
- Yali Zhang, assistant professor1 2 3,
- Jie Qiao, professor7 8 9,
- Jan Blustein, professor10 11,
- Jian-meng Liu, professor1 2 3 9
- 1Institute of Reproductive and Child Health, National Health Commission Key Laboratory of Reproductive Health, Peking University Health Science Centre, Beijing 100191, China
- 2Office for National Maternal and Child Health Statistics of China, School of Public Health, Peking University Health Science Centre, Beijing, China
- 3Department of Epidemiology and Biostatistics, School of Public Health, Peking University Health Science Centre, Beijing, China
- 4Centre for Health Statistics and Information, National Health Commission of China, Beijing, China
- 5Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
- 6Department of Maternal and Child Health, School of Public Health, Peking University Health Science Centre, Beijing, China
- 7Department of Obstetrics and Gynecology, Centre for Reproductive Medicine, Peking University Third Hospital, Beijing 100191, China
- 8Key Laboratory of Assisted Reproduction, Ministry of Education, Beijing, China
- 9Reproductive Health Research Centre, Peking University Health Science Centre, Beijing, China
- 10Robert F Wagner Graduate School of Public Service, New York University, New York, NY, USA
- 11Department of Population Health, School of Medicine, New York University, New York, NY, USA
- Correspondence to: J Liu liujm{at}pku.edu.cn; J Qiao jie.qiao{at}263.net
- Accepted 20 June 2019
Abstract
Objective To measure the association of China’s universal two child policy, announced in October 2015, with changes in births and health related birth characteristics.
Design National, descriptive before-and-after comparative study.
Setting Every county in 28 of 31 provinces of mainland China.
Participants Births included in two national databases: 67 786 749 births from county level monthly aggregated data between January 2014 and December 2017; and 31 786 279 deliveries from individual level delivery information records between January 2015 and December 2017.
Main outcome measures Monthly mean number of births and mean proportion of multiparous mothers and mothers aged 35 and over, preterm deliveries, and caesarean deliveries.
Results The study had two phases: the baseline period (up to and including June 2016, nine months after the policy announcement) and the effective period (from July 2016 to December 2017). The estimated number of additional births attributable to the new policy between July 2016 and December 2017 was 5.40 million (95% confidence interval 4.34 to 6.46). The monthly mean percentage of multiparous mothers and mothers aged 35 and over increased by 9.1 percentage points (95% confidence interval 6.4 to 11.7) and 5.8 percentage points (5.2 to 6.4), respectively. This increase in older mothers, however, was not associated with a concurrent increase in the overall rate of preterm birth. The monthly mean caesarean delivery rate among multiparous mothers increased by 1.2 percentage points (0.8 to 1.6) from 39.7% to 40.9%, and decreased by 3.0 percentage points (−3.5 to −2.5) among nulliparous mothers from 39.6% to 36.6%.
Conclusions Since its announcement in October 2015, the universal two child policy has been associated with a rise in births in China and with changes in health related birth characteristics: women giving birth have been more likely to be multiparous, and more likely to be aged 35 and over. No evidence of concurrent worsening outcomes (that is, premature births) was seen.
Introduction
China’s universal two child policy, announced in October 2015, was enacted to ameliorate the nation’s stagnant population growth, ageing population, and shrinking workforce. The policy targeted some 90 million women of reproductive age who had a previous delivery, and who would have been allowed to have a second child after October 2015.1 Although many people from western countries might consider China’s previous one child policy to be monolithic, the laws and practices governing fertility have varied greatly over time. As described elsewhere,234 shortly after the one child policy was introduced in 1979, couples in some rural areas were permitted to have two children if the first child was female. Subsequently, families in which both parents were only children were allowed to have a second child. From November 2013, couples were allowed to have a second child if either parent was an only child (the selective two child policy).4
Fertility in China has long been driven by factors beyond governmental rules. Most births occur in the early winter, about nine months after families reunite for the annual spring festival.5 Superstition also affects timing: a particularly unlucky time is considered to be the year of the sheep in the Chinese calendar, which brings about a substantial drop in births.6 A third determinant is economic: surveys show that many Chinese couples defer childbearing because of expense, particularly those living in large cities.78
The impact of the universal two child policy in China has had much speculation. Firstly, the goal was to increase the number of births, and projections have ranged from about one million to more than 10 million additional births annually.19 Secondly, concerns have been raised about maternal and child health stemming from a projected increase in births to older mothers, a higher risk population for many pregnancy complications and premature delivery.1011 Among the 90 million targeted women, an estimated 60% were over 35 and 50% over 40.1 Finally, the policy could have encouraged first time mothers to have a vaginal delivery instead of an elective caesarean delivery in anticipation of a future second birth.12 Elective primary caesarean delivery was the most common reason for caesarean section in the one child policy era, owing to many factors including the belief in the relative safety of caesareans when the intended family size was one child.13 Various Chinese health policies have aimed to reduce caesarean rates, including a brief time in 2015-16 when hospitals were rewarded for low caesarean rates.14 The primary objective of this study was to estimate the number of additional births that were attributable to the universal two child policy change. In addition, we aimed to describe changes in the health related characteristics of births following the policy change.
Methods
Data sources
We used two data sources compiled according to regulations issued by the National Health Commission of China: county level monthly aggregated data (CMAD) and individual level delivery information records (IDIR).15 The CMAD dataset is collected by a network managed over the past 20 years by the Office for National Maternal and Child Health Statistics of China.16 The CMAD system, added to the Office for National Maternal and Child Health Statistics of China’s data reporting suite in January 2014, draws monthly aggregate reports of births directly from all hospitals in China (>99% of births in China are in hospitals).17 The CMAD, as described in a previous publication,6 is regarded as the ideal source of data on the total number of births nationwide.18
The IDIR dataset was launched in January 2015, just before the universal two child policy was introduced, via an already existing data reporting network operated by the Centre for Health Statistics and Information of China. IDIR data are reported from hospitals; non-hospital births are reported by township healthcare centres. A limited set of measures are collected, including maternal age, parity, mode of delivery (caesarean section v vaginal delivery), and gestational age at delivery (added subsequently in January 2016). The IDIR system currently captures about two thirds of the births in China. We discuss the representativeness of the IDIR database below.
Data extraction and cleaning
From the CMAD database, we retrieved monthly births from 1 January 2014 to 31 December 2017 for every county in mainland China, except those for counties from Tibet, Xinjiang, and Qinghai, three sparsely populated rural provinces where reporting is of variable reliability or incomplete and where an estimated 2.5% percent of births occur. After excluding 3159 (2.4%) records reporting zero births, 128 833 county months remained, with 67 786 749 births. The subset from 1 January 2015 to 31 December 2017 included 50 113 889 births.
Between January 2015 and December 2017, the IDIR database had 31 786 279 delivery records from 28 of 31 provinces in mainland China (again, Tibet, Xinjiang, and Qinghai were excluded). Of these, 53 662 (0.17%) deliveries occurred out of hospital. We identified missing or likely incorrect data on maternal age at delivery (age <13.0 or ≥50.0) in 0.38% (n=120 561) of the records, missing data on delivery mode in 0.03% (n=9856), and missing data on parity in 4.4% (n=1 404 980). Between January 2016 and December 2017, the IDIR database had 23 077 074 delivery records, of which 5.9% (n=1 360 748) had missing or likely incorrect data of gestational age (<28 or >50 weeks). Preterm delivery was defined as delivery occurring between 28 and less than 37 completed weeks of gestation. However, the relatively higher percentage of missing or likely incorrect data on parity and gestational age were primarily driven by data from Hebei province; the corresponding percentage for the remaining 27 provinces was 0.01% and 1.19%, respectively.
Analysis
Displaying temporal patterns in total monthly births
We charted the number of births by month in the CMAD data to visualise patterns of seasonality,5 any drops in births during the year of the sheep (19 February 2015 to 7 February 2016),6 and potential responses to the selective and universal two child policies.
Assessing representativeness of IDIR data
We compared the numbers of monthly births in the CMAD and IDIR databases from January 2015 to December 2017 in visual displays and assessed any concordance between monthly births using the Pearson correlation coefficient. We explored the representativeness of the IDIR data by examining whether births reported to the IDIR, relative to births in CMAD, disproportionately came from rural or urban areas, or from areas of varying stringency of fertility policies before the universal two child policy, using the taxonomy developed by Gu and colleagues,2 in which provinces were classified as most restrictive, moderately restrictive, and least restrictive.
Estimating total multiparous and nulliparous births
Although the CMAD database is a complete report on numbers of births, it does not include information about births, such as whether those births were to nulliparous or multiparous mothers. To overcome this limitation, we calculated the monthly percentage of nulliparous and multiparous deliveries in the IDIR data and applied those percentages to the total births for that month in the CMAD database. This approach yielded monthly estimates of the number of nulliparous and multiparous births nationwide.
Estimating additional births attributable to the policy change
We examined monthly trends in estimated nulliparous and multiparous births in the CMAD data to assess whether births in the two groups followed parallel trends during the baseline period (that is, from the start of the data series to nine months after the announcement of the universal two child policy (June 2016)), but diverged during the effective period (July 2016 to December 2017). We used a difference-in-difference approach, which estimates the effect of a specific intervention (that is, policy change) by comparing the change in mean outcomes over time (that is, before and after the policy intervention) between a population that is affected by the intervention and a population that is not,19 to estimate births attributable to the policy. We assumed that nulliparous births were not affected by the universal two child policy and that multiparous births and nulliparous births would have continued to trend in parallel had the universal two child policy not been introduced. Our model was: Yt=β0+(β1×policyt)+(β2×parityt)+(β3×policyt×parityt)+(β4×month dummyt)+et.
Here, Yt is the number of births in month t. Policy is a variable indicating whether the observation was during the effective period (coded as 0 for months before July 2016 and 1 for months thereafter). Parity is a variable indicating the type of births (coded as 0 for births to nulliparas and 1 for births to multiparas). Month dummy included a set of 11 indicators, representing the 12 calendar months of a year. The number of births in the nation as a whole was the unit of analysis for this model. The regression coefficient of the interaction term between policy and parity (β3) can be interpreted as the monthly mean number of births attributable to the universal two child policy. We found the total number of births attributable to the policy as 18×β3, where 18 represents the total number of months of the effective period.
Exploring any causal attribution of universal two child policy on characteristics of births
Using IDIR data, we tested whether two changes in the characteristics of births would be specifically caused by the universal two child policy: an increase in the percentage of deliveries to multiparous women, and an increase in the percentage of deliveries to women of advanced age (≥35 years). Changes in these rates quantify the extent to which the new policy was associated with changes in the characteristics of typical births. We could not find a logical comparison group against which to measure changes, so we could not use a difference-in-difference approach. Instead, we used interrupted time series models2021 with segmented regression specifications22 to quantify changes from the baseline period. Models were: Yt=β0+(β1×montht)+(β2×policyt)+(β3×month dummyt)+et.
Here, Yt is the percentage of mothers with the characteristic of interest, month is a continuous variable indicating time in months from the start of the observation period (coded as 1-36, January 2015 to December 2017). Policy is a variable indicating the universal two child policy (0 at baseline, increasing to 1 during the effective period). Our coding of the policy variable reflected visually apparent trends: the effective period showed a temporary change in slope followed by a sustained plateau. Here, we report estimates of β2, interpretable as the change in the level of the outcome (in percentage points) between the baseline period and the plateau portion of the effective period. Further details are in the supplement.
Assessing changes in other key maternal and neonatal health characteristics
We quantified the association of the universal two child policy with changes in the preterm delivery rate using the standard interrupted time series and segmented regression approach,2022 from which a level change as well as a change in the slope can be estimated (eText). We also examined the association in subgroups defined by parity (nulliparous v multiparous) and maternal age at delivery (≥35 v <35 years). We planned to examine caesarean delivery rates using the same approach (see below). All analyses were conducted by IBM SPSS Statistics 20.0.
Patient and public involvement
Neither patients nor the public were involved in the study design, analysis of data, or interpretation of study results. The results of this study will be disseminated via the media centre of the authors’ institutions and probably also via mass media.
Results
Temporal trends in total monthly births
From January 2014 to December 2017, 67.79 million births were reported to the CMAD system in the 28 Chinese provinces (mean 1.41 million births per month (standard deviation 0.17)). Visual inspection (fig 1) showed a marked seasonality, with births peaking in the winter. Births were relatively low during the year of the sheep (February 2015 to February 2016). Peaks were highest in the winters of 2014 (following the announcement of the selective two child policy in November 2013) and 2016 (following the announcement of the universal two child policy in October 2015).

Number of births in mainland China during January 2014 and December 2017, by month (information taken from county level monthly aggregated data). Both selective and universal two child policies were assumed to take effect about nine months after being announced. The year of the sheep in the Chinese calendar, falling between February 2015 and February 2016, is considered to be a particularly unlucky time of birth
{kind=link}
Representativeness of IDIR data
The monthly number of deliveries in the IDIR dataset from January 2015 to December 2017 closely paralleled CMAD monthly births (eFigure 1 in the supplement), and the correlation between them was high (r=0.88; P<0.001). Compared with the CMAD’s number of births (considered to be the most accurate representation), representation of rural (62.9%) and urban (63.8%) deliveries was nearly equal in the IDIR database. However, the IDIR database over-represented deliveries in provinces with the least restrictive policies before the universal two child policy (84.9%), compared with 69.7% of deliveries in provinces with the most restrictive policies and 60.8% of deliveries in provinces with moderately restrictive policies (eTable 1).
Estimation of births attributable to the policy change
During the baseline period, estimated births to multiparous mothers ran nearly parallel to, but were consistently lower than, estimated births to nulliparous mothers (fig 2). After June 2016, estimated births to multiparous mothers were consistently higher than those to nulliparous mothers. The difference-in-difference analysis yielded an estimate of 0.30 million additional monthly births (95% confidence interval 0.24 to 0.36) during the effective period, corresponding to a total of 5.40 (4.34 to 6.46) million births during the 18 month period (eTable 2 in the supplement shows model coefficients).

Number of births to nulliparous and multiparous mothers in mainland China, by month (January 2015 to December 2017). Births to nulliparous and multiparous mothers were estimated using the strategy described in the methods. Hypothetical births to multiparous mothers (that is, assuming that the policy had not been introduced) were calculated by subtracting the mean difference between births to nulliparous mothers and those to multiparous mothers during the baseline period (January 2015 to June 2016) from the number of nulliparous births at each month (July 2016 to December 2017)
{kind=link}
Changes in percentage of multiparous women and women at advanced maternal age
At baseline, the monthly percentage of multiparous deliveries in the IDIR dataset fluctuated around a mean of 46.4% (standard deviation 1.5%; fig 3). During the effective period, this percentage rose and then plateaued, levelling at an additional 9.1 percentage points (95% confidence interval 6.4 to 11.7) from the baseline at 55.5% by regression estimate (table 1). In other words, following the policy change, multiparous births became the norm in China. Further analyses showed that the increase was more pronounced in mothers who had delivered one baby before the current delivery (+8.0 percentage points, 95% confidence interval 4.6 to 11.3) than in those who had delivered two or more babies (+1.1, 0.1 to 2.2), supporting the specificity of the policy effect (eFigure 2). The monthly mean percentage of older mothers (≥35 years) fluctuated around a baseline mean of 8.5% (standard deviation 0.3%; fig 3). During the effective period, this percentage rose substantially by an additional 5.8 percentage points (95% confidence interval 5.2 to 6.4) and levelled at 14.3% by regression estimate (table 1).

Secular trends in percentage of multiparous mothers (top) and mothers aged 35 and over (bottom) in mainland China from January 2015 to December 2017, based on data from individual level delivery information records. Dotted yellow line=mean monthly percentage of multiparous mothers during January 2015 to June 2016 (46.4%; top) or mean monthly percentage of mothers aged 35 and older during January 2015 to June 2016 (8.5%; bottom)
{kind=link}
Levels and changes in levels in birth related health factors associated with China’s universal two child policy (announced in October 2015), based on data from individual level delivery information records (IDIR)
Changes in other key maternal and neonatal health characteristics
At baseline, we saw no difference in the monthly mean rate of preterm delivery between nulliparous (4.2% (standard deviation 0.3%)) and multiparous (4.2% (0.3%)) mothers (P=0.99), but the monthly mean rate was significantly higher among mothers aged 35 and older (6.8% (0.5%)) than among younger mothers (4.0% (0.3%); P<0.001). The increase in older mothers (a relatively high risk group) in the subsequent period, however, was not associated with a change either in the baseline monthly mean level (−0.01 percentage points, 95% confidence interval −0.49 to 0.46) or in the slope (−0.02, −0.16 to 0.11) of the overall preterm delivery rate, after we controlled for the baseline trends and seasonality using the interrupted times series and segmented regression analysis. Stratified analyses by parity and maternal age at delivery also showed no association of policy change with preterm delivery rate (eFigures 3a and 3b).
Visual inspection showed a trough in caesarean deliveries between August 2015 and March 2016 (fig 4), possibly due to the transient policy change mentioned above. During this period, the governmental health departments used the medically unnecessary caesarean delivery rate as a key indicator in a national campaign assessing hospitals’ so-called baby friendliness.14 Because the trough precluded the use of the segmented approach, we made simple pairwise comparisons between the baseline and plateau phase rates to estimate level changes. Among nulliparous women, the monthly mean caesarean delivery rate decreased over time, from 39.6% in January-June 2015 to 36.6% in February-December 2017 (P<0.001; table 1). For multiparous women, the monthly mean rate increased from 39.7% to 40.9% over the same period (P<0.001; table 1).

Monthly trends in overall and parity specific rates of caesarean delivery in mainland China, from January 2016 to December 2017, based on data from individual level delivery information records
{kind=link}
Discussion
Principal findings
By joint analysis of two national data sources, we estimated that China’s universal two child policy was associated with an additional 5.40 (95% confidence interval 4.34 to 6.46) million births to multiparous women during the first 18 months that it was in effect. The policy was also associated with an increase in the monthly percentage of multiparous mothers by 9.1 percentage points from a baseline mean level of 46.4%; following the policy change, multiparous births exceeded nulliparous births nationwide. The increases in births began about nine months after the announcement of the universal two child policy and were largely driven by births to mothers who had already delivered one baby, indicating that these increases are less likely to be a reflection of time period increase in population or an effect of cohort shift. During the one child policy era, if couples violated the policy to have a second child, their newborn child might have been unable to attain Hukou status and lose access to various social benefits (such as education and healthcare) as a result.23 With the universal two child policy, the improved legal status of the child and the ability to attain Hukou status could have encouraged couples to have a second child.
The universal two child policy was also associated with an increase in births to older mothers (age ≥35 years). Between the baseline period and the plateau phase, the monthly mean percentage of older women grew from 8.5% to 13.5% (a 58.8% increase). Despite this rise in an at-risk population, we saw no significant increase in preterm birth rates nationwide when controlling for the baseline trends and seasonality.
Finally, we saw a slight decrease in caesarean deliveries to nulliparous mothers, which might signal a favourable trend towards vaginal birth in first time mothers in China.12 This impact on the overall caesarean delivery rate could have been attenuated by increased caesarean deliveries in multiparous women in China, most likely repeat caesarean sections, because vaginal birth after caesarean sections is not generally available owing to safety concerns. However, many of the changes associated with the policy, including the increase in births, appeared to diminish at the end of the study period, raising questions about whether the policy’s effects will be sustained.
Limitations of this study
Our estimates were subject to several caveats, the first of which pertains to the validity and representativeness of the data. The IDIR data were our source for characteristics of births, and the database is an incomplete report of births. We know of no incentive for false reporting or failure to report on the part of hospitals. Reassuringly, we did not find an appreciable difference in the propensity to report by rural versus urban areas (an important distinction from the perspective of fertility). We found an elevated propensity to report from areas with the least restrictive previous fertility policies. Since those areas had the least robust response to the policy (detailed analyses not shown), this bias would likely underestimate the impact of the policy on births. Moreover, our difference-in-difference estimate is subject to the caveat that the data (numbers of births of each type in the CMAD data) were first estimated from proportions of each type in the IDIR data. Given that the estimated impact of the change due to the universal two child policy was highly significant, this double estimation issue is probably not a concern.
Another limitation was that we excluded three primarily rural provinces (Tibet, Xinjiang, and Qinghai) that account for about 2.5% of national deliveries in generally less developed areas and where caesarean rates are much lower.16 Therefore, we could have overestimated the caesarean section rate. Despite a lack of nationally representative estimates of preterm delivery rate in China, a comparative study suggested that China’s preterm delivery rate was much lower than western countries.24 The baseline rate of preterm delivery in our study at 4.2% was roughly consistent with this comparative study and also comparable with some other population based studies conducted in local settings of China,2526 although lower than WHO estimates,27 perhaps due to the difference in the definition of preterm delivery. Preterm delivery was defined as a delivery between 28 and less than 37 completed weeks of gestation in our study, and defined as a delivery occurring before 37 completed weeks of gestation (including extremely preterm deliveries less than 28 weeks) in the WHO study.
Changes in the structure of the population of women of childbearing age could also bias our estimate of additional births. Over the past three years, the demographics shifted slightly: the number of women aged 20-29 (the typical range for nulliparous mothers) fell by 3.0% from 169 million in January 2014-June 2015 to 164 million in July 2015-December 2016,28 but the percentage of women aged 25-34 years (the typical range for multiparous mothers), increased by 3.6% from 166 million to 172 million in the same time period. Neither of our estimates of total births takes this change into account, but the overestimate is probably relatively minor.
Finally, contemporaneous changes in fertility could have occurred that were unrelated to the policy change. Close analysis revealed an 18.6% decrease in nulliparous births from 2016 (8.75 million) to 2017 (7.12 million). We can only speculate as to the cause of this drop. If fertility desires for multiparous mothers and nulliparous mothers changed equally, then our difference-in-difference estimate is unbiased. If it disproportionately affected one group over another, the bias could have gone either way. If the drop in births to nulliparous mothers continues, its long term impact on China’s future demographics deserves close investigation, especially if associated with an increase in maternal age with the first birth.29
Conclusions and policy implications
This study reports on the early period following the implementation of China’s universal two child policy. The policy increased births at a level that was roughly consistent with a widely cited projection,1 but total births did not reach the highest annual target of 20 million.30 Even reaching this target of 20 million, the excess births associated with the universal two child policy would have limited impact on China’s long term demographic future, particularly on the anticipated workforce shrinkage in about 30 years, although the excess births could postpone the arrival of the negative population growth predicted by many demographers.3132 In April 2019, the Chinese government provided the national regulatory guidance on infant and child care to help encourage and facilitate families and mothers raising children.33 Whether that guidance will augment the response to the universal two child policy needs monitoring. Although the policy was not accompanied by significantly increased preterm births in this study, more work is needed to document and ensure the health of an increasingly older maternal population of second time mothers in a country where caesarean delivery rates are high. Further research is needed to develop a more nuanced understanding of the sustained impact of this historical change in China.
What is already known on this topic
In October 2015, the Chinese government announced the universal two child policy, permitting all couples to have two children
A handful of studies have assessed the changes in some health indicators following the introduction of the policy
However, these studies only drew from one or a few hospitals, with limited geographical coverage
What this study adds
In this study using national data to estimate the impact of the policy change, the number of births increased in the immediate period after the announcement of the policy, although not as much as some policy makers had expected
During the same period, the number of nationwide, multiparous births exceeded nulliparous births, a reversal of a longstanding pattern; births to older mothers (age ≥35) increased, but no accompanying increase in premature births was seen
The number of caesarean deliveries decreased for primiparous mothers, but rose slightly for mothers who had given birth previously
Acknowledgments
We thank the thousands of health workers who contributed to the collection of the two datasets and the tens of millions of people who supplied the data.
Footnotes
Contributors: HL, MX, SH, JQ, JB, and JL contributed to the conception and design of the study. JQ, JB, and JL provided overall guidance. HL, MX, YC, YG, and YZ contributed to data collection and cleaning. HL and MX did the analysis. HL, MX, SH, JQ, JB, and JL prepared the first draft. All authors reviewed the whole draft and approved the final manuscript. HL and MX are joint first authors. JQ and JL are joint corresponding authors. JQ and JL are the guarantors. The corresponding authors attest that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This study was supported by grants from the National Key Research and Development Program of China (2016YFC1000401, 2016YFC1000406-1), National Health Commission of China, and National Natural Science Foundation of China (81571517, 81701538). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report, and did not participate in the decision to submit the manuscript for publication.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Key Research and Development Program of China, National Health Commission of China, and National Natural Science Foundation of China for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was deemed exempt from the Peking University Health Science Centre’s institutional review board because it used previously collected data containing no personally identifiable information.
Data sharing: No additional data available.
The corresponding authors affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.