Determining the approximate area of a burn: an inconsistency investigated and re-evaluated
BMJ 1996; 312 doi: https://doi.org/10.1136/bmj.312.7042.1338 (Published 25 May 1996) Cite this as: BMJ 1996;312:1338
- R J Perry,
- C A Moore,
- B D G Morgan,
- D L Plummer
- University College London Medical School, Clinical Sciences Office, Administration, London WC1E 6BT Richard J Perry
- medical student Cheryl A Moore, medical student. Department of Plastic Surgery, University College London Hospitals, London WC1E 6BT
- Brian D G Morgan, consultant plastic surgeon. Department of Medical Physics and Bioengineering, University College London, London WC1E 6BT
- David L Plummer, medical physicist.
- Correspondence to: Mr Perry.
- Accepted 18 December 1995
For assessing the area of small or irregular burns a projection of the patient's whole hand is used as an approximation to 1% of the total body surface area.1 In the advanced trauma life support course manual,2 however, the palm (not including the fingers) has been quoted as representing 1%. This study was undertaken to determine which method is the better approximation.
Subjects, methods, and results
Twenty adults from the medical school and 10 children from the hospital took part in this project. Their heights (cm) and weights (kg) were recorded on calibrated equipment and their total body surface area was calculated by the method of Gehan and George.3 The projections of each subject's palm and whole hand were delineated using their non-dominant hand. The area of each projection was determined using the DispImage computer program.4
Among the adults the means of each individual's projected palm and whole hand areas expressed as a percentage of their total body surface area, with 95% confidence intervals, were 0.41 (0.39 to 0.43)% and 0.77 (0.74 to 0.80)% respectively. Among the children the corresponding values were 0.45 (0.42 to 0.48)% and 0.82 (0.78 to 0.87)% (fig 1). For the two groups combined the mean projected whole hand area was 0.79 (0.76 to 0.81)%.
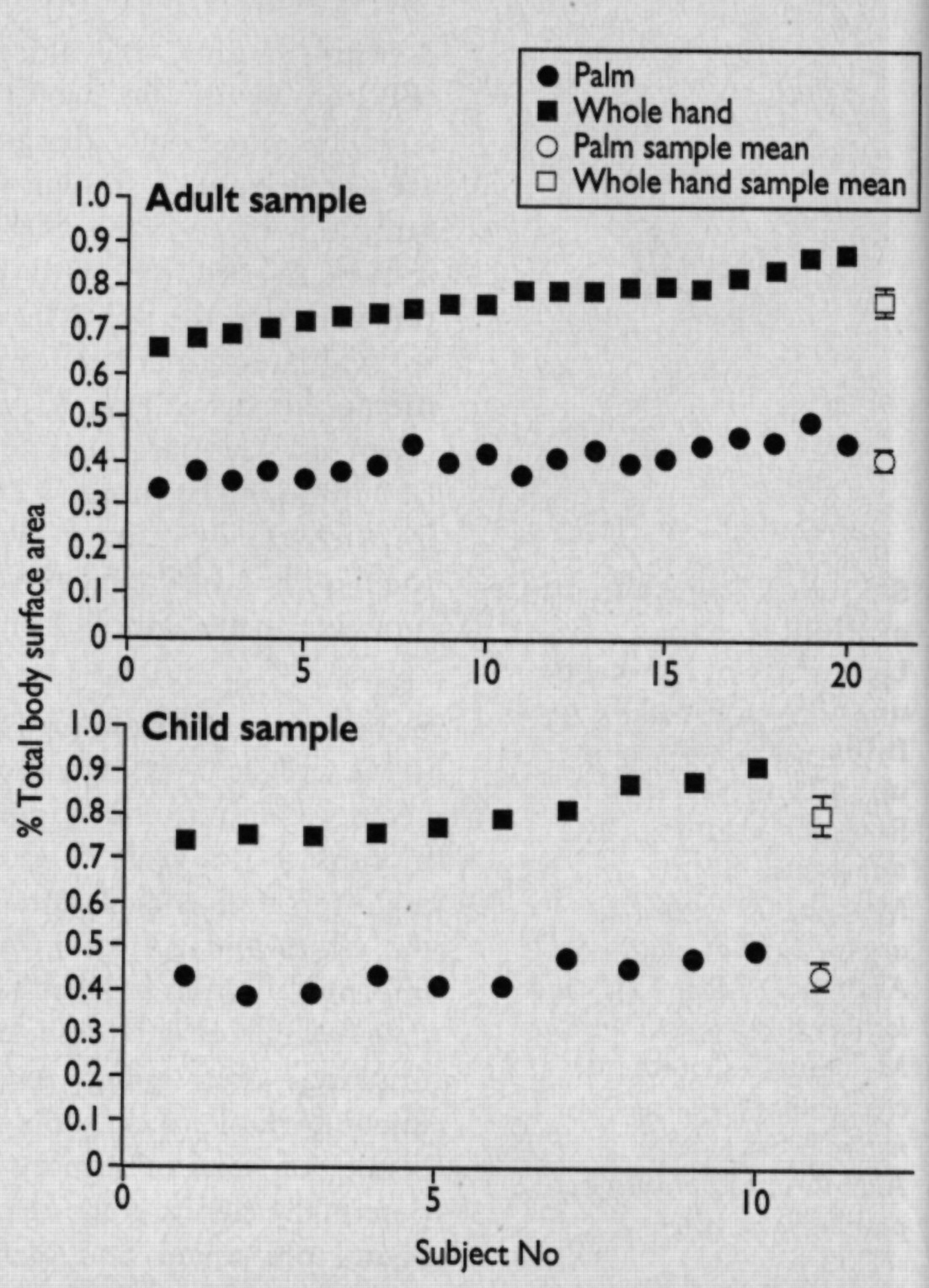
Plots of each individual's projected palm and whole hand area expressed as a percentage of their total body surface area together with means and 95% confidence intervals in adult and child groups
{kind=link}
Comment
The purpose of this investigation was to determine which of a person's projected palm or whole hand area is a better approximation to 1% of their total body surface area. The results (fig 1) clearly indicate that the whole hand and not the palm is the better measure, and this conclusion is not altered when all determinable errors are taken into account.
Although the subjects were from the hospital and medical school, they were from varying cultural and social backgrounds, and we feel they are representative of the general population for the variable being measured. The between observer variation was removed by the study design while the within observer variability was assessed to be about 6% for the projected palm and 4% for the projected whole hand areas.
The DuBois and DuBois formula is routinely used for calculating a subject's total body surface area. However, the constant powers used in this formula were determined by a study in only nine subjects.5 Subsequent larger studies have generated new values for these variables,3 which were used in this project.
In neither the adults nor the children did the 95% confidence interval for the mean of the projected whole hand area contain the 1% value it is supposed to be approximating. Hence, we propose that the projected whole hand should be taken to approximate to 0.8% of total body surface area, the actual mean value for the combined groups (0.79%) being too cumbersome for easy calculations. We also propose that this new value should be used for both adults and children because, although the means of the adult and child samples did differ significantly (0.05 > P > 0.02 for the null hypothesis), this difference is too small to affect the overall conclusion.
Consistency in determining the area of a burn would allow more accurate comparison of results of treatment protocols between hospitals. Achieving consistency between hospitals is often difficult, but within a hospital consistency can be obtained by a unit basing its burns admission policy and treatment protocol on one documented method of approximating the area of tissue damage which is known to all staff.
We thank all the people who participated in this study and Eric Brunner, Jenny Head, Mark Holmes, Julie Moore, and Karen Perry for their help and advice with this investigation.
Footnotes
-
Funding None.
-
Conflict of interest None.