General practice based intervention to prevent repeat episodes of deliberate self harm: cluster randomised controlled trial
BMJ 2002; 324 doi: https://doi.org/10.1136/bmj.324.7348.1254 (Published 25 May 2002) Cite this as: BMJ 2002;324:1254
- Olive Bennewith, research associatea,
- Nigel Stocks, clinical lecturera,
- David Gunnell, senior lecturer in epidemiology and public healthb,
- Tim J Peters, reader in medical statisticsb,
- Mark O Evans, lecturer in psychiatryc,
- Deborah J Sharp (debbie.sharp{at}bristol.ac.uk), professor of primary carea
- a Division of Primary Health Care, University of Bristol, Bristol BS6 6JL
- b Department of Social Medicine, University of Bristol
- c Division of Psychiatry, University of Bristol
- University of Liverpool, Royal Liverpool Hospital, Liverpool L69 3GA
- Correspondence to: D Sharp
- Accepted 29 August 2001
Abstract
Objectives: To evaluate the impact of an intervention based in general practice on the incidence of repeat episodes of deliberate self harm.
Design: Cluster randomised controlled trial in which 98 general practices were assigned in equal numbers to an intervention or a control group. The intervention comprised a letter from the general practitioner inviting the patient to consult, and guidelines on assessment and management of deliberate self harm for the general practitioner to use in consultations. Control patients received usual general practitioner care.
Setting: General practices within Avon, Wiltshire, and Somerset Health Authorities, whose patients lived within the catchment area of four general hospitals in Bristol and Bath.
Participants: 1932 patients registered with the study practices who had attended accident and emergency departments at one of the four hospitals after an episode of deliberate self harm.
Main outcome measures: Primary outcome was occurrence of a repeat episode of deliberate self harm in the 12 months after the index episode. Secondary outcomes were number of repeat episodes and time to first repeat.
Results: The incidence of repeat episodes of deliberate self harm was not significantly different for patients in the intervention group compared with the control group (odds ratio 1.2, 95% confidence interval 0.9 to 1.5). Similar findings were obtained for the number of repeat episodes and time to first repeat. Subgroup analyses indicated that there was no differential effect of the intervention according to patient's sex (P=0.51) or method used to cause deliberate self harm (P=0.64). The treatment seemed to be beneficial for people with a history of deliberate self harm, but it was associated with an adverse effect in people for whom the index episode was their first episode (interaction P=0.017).
Conclusions: An invitation to consult, sent by the general practitioner of patients who have deliberately harmed themselves, and the use of management guidelines during any subsequent consultation did not reduce the incidence of repeat self harm. A subgroup analysis that indicated that patients who had previously harmed themselves benefited from the intervention was inconsistent with previous evidence and should be treated with caution. More research is needed on how to manage patients who deliberately harm themselves, to reduce the incidence of repeat episodes.
What is already known on this topic
What is already known on this topic About two thirds of patients consult their general practitioner in the three months after an episode of deliberate self harm
There have been no previous large scale randomised controlled trials of general practice based interventions aimed at reducing the incidence of repeat episodes of deliberate self harm
What this study adds
What this study adds An intervention comprising an invitation to consult from a patient's general practitioner and by the use of guidelines for the assessment and management of deliberate self harm in a subsequent consultation does not reduce the incidence of repeat episodes of deliberate self harm
Introduction
Deliberate self harm is a serious clinical problem in England and Wales, accounting for an estimated 140 000 hospital presentations each year.1 The importance of this behaviour is emphasised further by two related consequences. Firstly, 15-23% of patients will be seen for treatment of a subsequent episode of deliberate self harm within one year. 2 3 Secondly, 3-5% of those who harm themselves die by suicide within 5-10 years.4
Evidence on how best to manage patients who have deliberately harmed themselves is lacking.5 Although studies have shown that about two thirds of patients who deliberately harm themselves visit their general practitioner within 4-12 weeks of the episode, 6 7 all previous evaluations of interventions to reduce repeat episodes have been based in secondary care.5
We examined the effectiveness of an intervention based in primary care, aimed at reducing the incidence of repeated deliberate self harm. The intervention comprised a letter from the general practitioner inviting the patient to make an appointment to consult, and guidelines on assessing and managing patients for the general practitioner to use in any subsequent consultation.
Methods
Protocol
Recruitment of practices—We received approval from the relevant research ethics committees. We contacted practices based in the areas covered by the Avon, Wiltshire, and Somerset Health Authorities whose patients lived within the catchment areas of four general hospitals: Bristol Royal Infirmary, Southmead Hospital, and Frenchay Hospital in Bristol, and the Royal United Hospital in Bath. We included 98 (60%) of the 162 practices eligible to participate in the trial. In total, 49 practices were allocated to the intervention arm and 49 to the control arm (fig 1). All communication between the trial team and practices was by post and telephone.

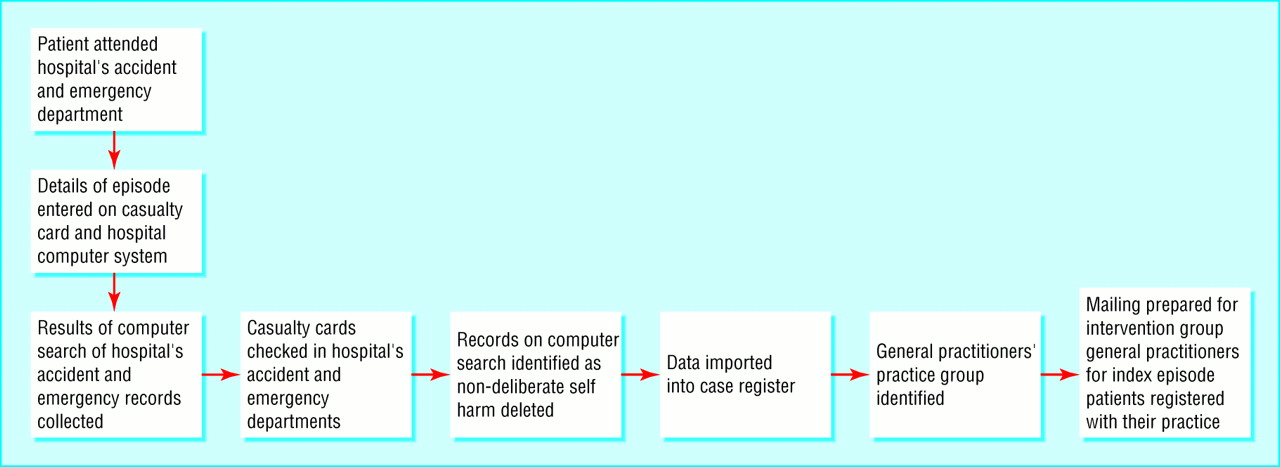
Recruitment of patients—We identified patients eligible for inclusion in the trial from a case register for deliberate self harm that covered Avon and part of Wiltshire. Recruitment data were collected on a weekly basis from the records of the hospitals' accident and emergency departments between 26 May 1997 and 29 February 1999 (fig 2). An episode of deliberate self harm was identified if the hospital's medical notes confirmed that the act had been deliberate and not fatal, had been done in the knowledge that it was potentially harmful, and, in the case of drug overdose, that the amount of drug taken was excessive. Audits showed that around 95% of all patients in the intervention and control groups who were subsequently admitted as inpatients (about half the total) were identified and recruited.

{kind=link}
{kind=link}
Exclusions—We excluded cases of alcohol (taken alone) and illicit drug overdose, except where the casualty officer felt that the purpose of the act was self harm or suicide. We excluded patients who were under 16, of no fixed abode, or imprisoned; who had requested that nobody was to be informed of the episode or had harmed themselves deliberately in response to a psychotic hallucination or delusion; or whose episode of deliberate self harm was managed entirely in primary care.
Intervention—At the start of each week, we identified new episodes of deliberate self harm in patients registered with practices in the intervention arm from the deliberate self harm case register. If an episode of deliberate self harm was the patient's first within the trial period, their general practitioner was sent a letter informing them of the incident, a letter to forward to the patient (at their discretion) inviting them to make an appointment for a consultation, and a copy of guidelines for the management of deliberate self harm, which were developed for the trial (see fig 3). The general practitioners were asked to insert the guidelines into the patient's notes so that they were available for use during consultation. Each general practitioner in the intervention arm was sent a copy of the guidelines at the start of the trial. We developed these guidelines using a formal consensus method—the modified Delphi technique—as there is no evidence from randomised controlled trials on the appropriate aftercare for deliberate self harm in general practice. The consensus group comprised general practitioners with an interest in mental health, psychiatrists, a psychologist, a specialist nurse, a voluntary worker from the Samaritans, and patients with a history of deliberate self harm. The research team synthesised the views of the consensus group to produce the final version of the guidelines.8

Assessment and management guidelines for deliberate self harm
{kind=link}
Usual care—With the exception of the Royal United Hospital, Bath (where a specialist nurse had been appointed), there were no specialist services for patients who deliberately harm themselves in the hospitals from which patients were recruited. To obtain more detailed information on usual care, we used two sources of information: (a) a postal questionnaire was sent to eight practices in the control group to obtain information on communications between hospital healthcare professionals and general practitioners that may have assisted in subsequent patient management; (b) hospital trusts and general practices were asked to provide data on referrals to mental health services in the 12 months following the index episode for a sample of 185 patients recruited over a six month period to the control arm of the trial.
Primary and secondary outcomes—The primary outcome measure for the trial was the occurrence of a repeat episode of deliberate self harm in the 12 months after the index episode. Secondary outcomes were the time (days) to the first repeat episode and the number of repeats.
Process data—We sent a postal questionnaire to all general practitioners to obtain information about the occurrence and timing of the first consultation during the 12 months after the index episode and the forwarding of the letter sent to the patient (intervention arm) or the instigation of patient contact by the general practitioner (control arm). This questionnaire was followed up with telephone reminders. We assessed contamination resulting from patients moving to another practice (particularly between trial arms) and loss to follow up through patients moving out of the area (resulting in loss of information on repetition of deliberate self harm) for 178 consecutive recruits to the intervention and control groups during weeks 50-60 of the trial.
Sample size calculation—We needed 1920 patients to detect a reduction of five percentage points (from 15% to 10%) in the rate of repeat deliberate self harm in 12 months (giving 80% power, 5% significance level, and 40% inflation to allow for the cluster randomisation by practice). The inflation factor was calculated by using data about the size of practice populations and about admissions for deliberate self harm for practices in Avon between 1992 and 1993.9
Data analyses
We carried out statistical analyses in accordance with CONSORT guideline, using Stata version 6.0. For the primary analysis, which compared the intervention and control groups on an intention to treat basis, we carried out a logistic regression analysis with repeat episodes of deliberate self harm within 12 months of the index event as the outcome variable. This analysis controlled for practice size (two categories) and quartile of rates of deliberate self harm by practice at baseline and allowed for clustering by practice, using random effects logistic regression.
We used a Poisson regression analysis to compare the intervention and control groups in terms of differences in the number of repeat episodes. We used Cox's proportional hazards regression for time (in days) to first repeat episode. Clustering was taken into account for both of these (intention to treat) analyses.
Further regression analyses adjusted for factors with large baseline differences across randomisation groups. An explanatory analysis, excluding two groups of patients, was also carried out. Firstly, we removed patients who had a repeat episode of deliberate self harm within 14 days of the index episode—before those in the intervention group could have received and responded to the intervention letter—from both groups. Secondly, we excluded patients from the intervention group for whom a letter was not sent to the general practitioner.
We performed subgroup analyses, agreed on before the trial began, using interaction terms to assess whether the intervention effect on the primary outcome differed according to sex, method of deliberate self harm, and previously recorded episodes of deliberate self harm. The same approach was used for one post hoc subgroup analysis to investigate differential effects according to whether or not the patients used drugs prescribed for a mental health problem, since this might reflect an established relationship with the general practitioner in respect of such problems. Data about previously recorded episodes of deliberate self harm were available for patients attending the hospital in Bath for only 14 weeks compared with 2.5 years for patients attending the hospitals in Bristol.
For process data, descriptive statistics were used to assess patterns of consultation after the index episode, use of the intervention letter, and details of usual care.
Assignment—Practices were stratified into four groups, according to the rate of deliberate self harm. To maximise comparability with respect to the availability of mental health services based in the practices that might be related to practice size and the number of individual patients across the arms of the trial, each of the four groups was divided into two further groups according to practice size (fewer than four general practitioners and four or more general practitioners). Within these eight strata, practices were allocated to intervention or control groups, using random number tables, by people blind to the practices' identities (TJP and Angela Liebenau).
Masking—The trial arm was identified after OB judged whether or not the episode met the study's definition of deliberate self harm. Although the general practitioner's name was included in the list of fields displayed in the computer printout, the assessment was made blind to direct knowledge of the randomisation group. Because of the nature of the trial, general practitioners were not blind to the patients' allocations.
Results
In total, 2084 potentially eligible patients were identified over the 21 month period of recruitment. We excluded 152 of these (fig 1).
Non-participating practices tended to be smaller and were less likely to be training practices than the participating practices. Fewer general practitioners in the non-participating practices had a postgraduate qualification or were fellows of the Royal College of General Practitioners (table 1). On the basis of the total catchment area for the practices in Avon, Townsend deprivation scores10 were similar for participating practices (mean −0.32; SD 0.74, 95% confidence interval −1.20 to 3.62) and non-participating practices (−0.16; 0.99, −1.23 to 3.07). Patient characteristics were comparable for the participating and non-participating practices (table 2). Although the control group had fewer training practices than the intervention group, other practice characteristics were reasonably well balanced between the trial arms (table 1).
Characteristics of practices and general practitioners
Characteristics of patients in intervention, control, and non-participating practices. Values are numbers (percentages) unless otherwise specified
Patient characteristics in the intervention and control groups differed for a recent recorded episode of deliberate self harm, general practice Townsend score (weighted by the number of patients recruited from each practice), and hospital attended for the index episode (table 2). The Royal United Hospital in Bath contributed more patients to the control group than in the intervention group (table 2).
Primary analysis
The proportion of participants who had a repeat episode of deliberate self harm within 12 months of the index episode was slightly higher in the intervention group (table 3). Logistic regression analysis for this primary outcome indicated that this comparison was not significant (odds ratio 1.17 (0.94 to 1.47) for the intervention group compared with the control group).
Repeat episodes of deliberate self harm within 12 months of index episode
The results were not noticeably different when we adjusted for clustering. The overall observed intra-practice correlation coefficient was only 0.006; little difference was seen between the randomised groups. This (observed) degree of clustering would have led to an inflation factor of 11% rather than the 40% that was estimated in the sample size calculation.
Secondary analyses
Although more repeat episodes of deliberate self harm and fewer days to first repeat episode were seen in the intervention group than in the control group, Poisson and Cox regression analyses showed that these differences were not significant (table 3). When we also adjusted for the practice's training status, previous recorded episodes of deliberate self harm, Townsend score, and hospital attended by the patient, no appreciable impact on the result for the primary outcome was seen (odds ratio 1.14, 0.88 to 1.50). Results were similar to the primary (intention to treat) analysis after patients who had deliberately harmed themselves within 14 days of the index episode and those whose general practitioners were not sent the intervention letter were excluded (1.25, 0.95 to 1.57).
Subgroup analyses
Subgroup analyses showed that the intervention effect did not differ by sex (interaction P=0.51) or method of deliberate self harm (interaction P=0.64). A similar analysis showed that the treatment effect differed depending on whether or not the patient had a previous recorded episode of deliberate self harm (interaction P=0.017). The odds ratio for the effect of intervention in patients with a history of deliberate self harm was 0.57 (0.33 to 0.98), indicating a beneficial effect, and in those with no history was 1.32 (1.02 to 1.70), indicating a harmful effect. Since only limited data were available about previous episodes of deliberate self harm for patients from the hospital in Bath, the analysis was repeated with all patients from this hospital omitted (approximately one third of the total); the interaction for previous episodes of deliberate self harm remained virtually unaltered. The post hoc subgroup analysis showed no differential effects according to whether or not the patient used an overdose of a drug likely to have been prescribed for a mental health problem (P=0.84).
Analyses of process data
Information about contact with the patient (letter, consultation, or both) was obtained from questionnaires completed by general practitioners for 1383 (72%) patients. Of 612 patients in the intervention group for whom the relevant information was provided, 352 (58%) had been sent the letter inviting them to make an appointment for a consultation. General practitioners in the control group had initiated contact with only 97/642 (15.1%) patients. In both groups, nearly 60% of patients had attended a consultation within six weeks of the index episode (intervention 351/599 (58.6%), control 387/681 (56.9%)). More than two thirds of these had attended within two weeks of the index episode (intervention 239/351 (68%), control 308/387 (80%)).
In a sample of 178 patients, a greater proportion of patients in the control group left their practice than in the intervention group during the 12 months after the index episode of deliberate self harm (76 (20%) v 102 (8%)). Of these, six (8%) patients moved from a control practice to an intervention practice and five (5%) from an intervention practice to a control practice. Few patients moved out of the study area: three (4%) and two (2%), respectively, for the control and intervention groups.
Usual care
The hospital the patient had attended generally provided general practitioners in the control arm with no structured feedback about patient management. In a sample of 185 patients in the control group, 74 (40%) were referred for psychiatric or community mental health team care or for counselling in the 12 months after the index episode.
Discussion
We believe that this is the largest trial of the management of deliberate self harm carried out and the only study based completely in primary care. Recruitment was from a wide range of patient groups. Although we excluded patients whose episode of deliberate self harm was managed entirely within primary care, over 95% of episodes of deliberate self harm involve an attendance at a hospital's accident and emergency department.11 Analysis of the characteristics of participating and non-participating practices and their patients showed that training practices and larger practices were more likely to take part in the trial. This may have meant that patients in control practices were already receiving better care than that generally received by patients in the area as a whole; this could have limited the capacity of the intervention to produce an improvement in outcome.
The intervention had no significant effect on patterns of repetition of deliberate self harm. If anything, the risk of repetition was slightly higher in the intervention group than in the control group. Although the confidence intervals around the odds ratio are fairly wide, they do exclude any important clinical benefit from the intervention.
Some evidence showed that the effects of the intervention were influenced by whether or not the subject had previously harmed themselves deliberately. Specifically, there seemed to be some benefit for the 14% of patients in the intervention group who had deliberately harmed themselves in the 2.5 years before the trial began. This subgroup effect should be treated with caution for several reasons. Firstly, the effect was in the opposite direction to that found in an earlier study in which patients with a history of deliberate self harm were less likely to benefit from being given a “green card” that offered them open access to psychiatric services in times of crisis.12 Secondly, the proportion of patients with a history of deliberate self harm was lower than anticipated from previous studies 1 13 because of the limited period of time for which data on previous episodes of deliberate self harm were collected. Full information on a history of deliberate self harm was available for only two thirds of patients (that is, not for patients from the Royal United Hospital). With these caveats in mind, it may be that patients in the trial who experienced care from their general practitioner better than that experienced after previous episodes were more willing to turn to their general practitioner for help in subsequent crises. This finding needs to be replicated.
Limitations of the trial
The development of guidelines to be given to general practitioners had to rely largely on existing opinion on best practice and on research on the assessment and management of problems known to be associated with deliberate self harm. In line with evidence from the literature that was available when we planned the study, the guidelines included information relevant to local circumstances and acted as a patient specific reminder. They were not disseminated with an active educational intervention.13 Deliberate self harm is a relatively rare event for each general practitioner—the rate of deliberate self harm in the general population is approximately 30 per 10 000 per year; on average, a general practitioner will encounter six new cases per year.14 In our study, the mean annual number of patients recruited per general practitioner was about three. It was thought unlikely that all general practitioners in the intervention arm could be attracted to attend specific educational sessions. Furthermore, a recent study using a practice based educational programme for depression—a much more common disorder—failed to change doctors' behaviour appreciably.15 Our guidelines probably enhanced the routine primary care of deliberate self harm because general practitioners have relatively little formal training in its management.
Though only a short delay occurred between the index episode and the general practitioner receiving the letter and guidelines, many patients had already consulted their general practitioner. This delay may be critical when we consider the increased risk of repeat episodes in the weeks immediately after the index event; in one study more than 10% of patients who deliberately harmed themselves again did so within one week of the index episode.16 Nevertheless, more general practitioners in the intervention group had initiated contact with their patients in response to the index episode of deliberate self harm than in the control group. All general practitioners in the intervention arm received copies of the guidelines at the outset of the trial and once a patient who deliberately harmed himself or herself had been identified. Receipt of the guidelines for previous patients may have influenced the management of “early attending” patients, even if the general practitioner had not received the guidelines and letter for that particular patient.
Our trial was pragmatic; the obstacles to its potential success were those that would arise if such a system was introduced in the service setting. Nevertheless, the implementation of the intervention showed that a more efficient form of communication with general practitioners is needed. An intervention aimed at reducing the incidence of repeat episodes of deliberate self harm must be initiated within one or two days of the index episode, because of the rate of repetition in this period and because help from general practitioners may already have been sought. Although the letter seems to have had little effect in instigating face to face contact between the patient and general practitioner, this may have been because of the delay in sending it to the patient. Where the letter had not resulted in the patient making contact with the general practitioner in the short term, their awareness of the interest shown by the general practitioner may have led them to seek help in future crises.
Conclusion
The lack of benefit from the intervention evaluated in this trial leaves open the question of the most effective management in general practice of patients with self harm. The role of the general practitioner in the aftercare of patients who deliberately harm themselves is important, as more than half of these patients receive no psychiatric follow up. The high proportion of patients who make contact with general practitioners after an episode of deliberate self harm suggests that more research is needed on how best to manage such patients in primary care to reduce the incidence of repeated episodes.
Acknowledgments
We thank the members of the consensus panel for the development of the guidelines: L Appleby, R Blacker, M Crawford, J Evans, P Evans, D Goldberg, A Harrison, K Hawton, A House, M Hunt, E King, G Lewis, M Moore, G Morgan, J Neeleman, R Paxton, D Russell, P Seager, and the Samaritans; the seven patients who helped develop the guidelines by agreeing to be interviewed on the day after their admission for deliberate self harm; the general practitioners, their secretaries, and practice managers; Avon, Wiltshire, and Somerset Health Authorities, the clinical directors, secretaries, and reception staff at Accident and Emergency departments; staff at the information technology departments at Bristol Royal Infirmary, Bath Royal United Hospital, Southmead Hospital, and Frenchay Hospitals; and staff at the United Bristol Health Trust Research and Development Support Unit for their help with data collection. We thank Angela Liebenau who was involved in the setting up of the trial and Kate Baxter and Maggie Evans for help with some of the process data. We also acknowledge the contribution of Dr Bill Bruce-Jones, consultant psychiatrist, to the design of the project.
Footnotes
-
Contributors DG, TJP, and DJS initiated the study. OB, NS, DG, TJP, MOE, and DJS designed the study. OB and NS contributed to data collection. OB, DG, and TJP analysed the data. OB wrote the first draft of the paper. NS, DG, TJP, and DJS contributed to and edited the paper. MOE edited the paper. DJS and OB will act as guarantors for the paper.
-
Funding National Health Service Executive South West Research and Development Directorate.
-
Competing interests None declared.
References
Commentary: Clinical guidelines have limitations
- Richard Morriss (rmorris{at}liverpool.ac.uk), professor of psychiatry
- a Division of Primary Health Care, University of Bristol, Bristol BS6 6JL
- b Department of Social Medicine, University of Bristol
- c Division of Psychiatry, University of Bristol
- University of Liverpool, Royal Liverpool Hospital, Liverpool L69 3GA
Bennewith et al provide further evidence that the provision of centrally derived clinical guidelines to general practitioners may be insufficient to improve the outcome of patients with mental health problems. The problems with the intervention in Bennewith et al's trial amount to more than how quickly guidelines to prevent deliberate self harm were sent to general practitioners. The intervention resulted in many more interviews with patients who committed deliberate self harm being initiated by general practitioners, but just as many patients who deliberately harmed themselves consulted their general practitioners and received mental health care in the group of patients who received usual treatment. Did the trial change the management of patients in the control group so that general practitioners referred more patients for mental health care to prevent suicide as a result of increased awareness surrounding the research? Did the hospitals routinely tell the patients to seek help from their general practitioners or to ask their general practitioners for a referral for mental health care? Are the patients who were seen by general practitioners or mental health providers in the intervention and control groups the patients at highest risk of episodes of deliberate self harm in the future?
The data from Bennewith et al suggest that the conclusions of a systematic review on changing doctors' behaviour,1 and, more specifically, a review about improving the mental health skills of general practitioners,2 are sound. Centrally derived guidelines can improve knowledge and remind doctors about aspects of practice with which they have previously been familiar. However, guidelines may have a modest effect on changing the doctor's performance, especially when the doctor needs to develop technical skills, the doctor is not confident about how to implement the guidelines, or the guidelines do not fit easily with the doctor's usual practice. The intervention for deliberate self harm in the appendix (see bmj.com) for the study by Bennewith et al requires advanced communication and mental health management skills from the doctor. Centrally derived guidelines do not give models on how to use these skills, opportunities to practice them under supervision, or opportunities for general practitioners to explore how they might be compatible with their perception of the needs of the patient and their usual practice.2 model of providing skills based training to improve the primary care team's assessment and management of people at risk of suicide, using academic detailing to deliver the training at a time and place convenient to the team, has been shown to be feasible3; a similar form of educational intervention showed lasting improvements in the management of health problems in adolescents.4
A final note of caution stems from another recent trial showing that only 22% of episodes of deliberate self harm resulted in treatment at accident and emergency departments.5 Unsuspected outcomes of interventions for deliberate self harm, including suicide, may be missed if studies do not include patients whose episodes of deliberate self harm do not result in hospital care.