Systematic review and meta-analysis of evidence for increasing numbers of drugs in antiretroviral combination therapy
BMJ 2002; 324 doi: https://doi.org/10.1136/bmj.324.7340.757 (Published 30 March 2002) Cite this as: BMJ 2002;324:757
- Rachel Jordan, senior scientist (r.e.jordan{at}bham.ac.uk)a,
- Lisa Gold, lecturerb,
- Carole Cummins, senior lecturerc,
- Chris Hyde, senior clinical lecturerd
- a CDSC (West Midlands), Department of Public Health and Epidemiology, University of Birmingham, Edgbaston, Birmingham B15 2TT
- b Health Economics Facility, Health Services Management Centre, University of Birmingham, Edgbaston, Birmingham B15 2RT
- c Institute of Child Health, University of Birmingham, Birmingham B4 6NH
- d Department of Public Health and Epidemiology, University of Birmingham, Edgbaston, Birmingham B15 2TT
- Correspondence to: R Jordan
- Accepted 7 November 2001
Abstract
Objective: To assess the evidence for the effectiveness of increasing numbers of drugs in antiretroviral combination therapy.
Design: Systematic review, meta-analysis, and meta-regression of fully reported randomised controlled trials. All studies included compared quadruple versus triple therapy, triple versus double therapy, double versus monotherapy, or monotherapy versus placebo or no treatment.
Participants: Patients with any stage of HIV infection who had not received antiretroviral therapy.
Main outcome measures: Changes in disease progression or death (clinical outcomes); CD4 count and plasma viral load (surrogate markers).
Search strategy: Six electronic databases, including Medline, Embase, and the Cochrane Library, searched up to February 2001.
Results: 54 randomised controlled trials, most of good quality, with 66 comparison groups were included in the analysis. For both the clinical outcomes and surrogate markers, combinations with up to and including three (triple therapy) were progressively and significantly more effective. The odds ratio for disease progression or death for triple therapy compared with double therapy was 0.6 (95% confidence interval 0.5 to 0.8). Heterogeneity in effect sizes was present in many outcomes but was largely related to the drugs used and trial quality.
Conclusions: Evidence from randomised controlled trials supports the use of triple therapy. Research is needed on the effectiveness of quadruple therapies and the relative effectiveness of specific combinations of drugs.
What is already known on this topic
What is already known on this topic Triple combination antiretroviral therapy is accepted by clinicians and patients as the usual treatment for HIV and has evolved through an incremental strategy in the numbers of drugs combined
Guidance on treatment, however, has predominantly been based on early reports of research
There are no published analyses that assess the effectiveness of the increasing numbers of drugs used in combination
What this study adds
What this study adds The results of this systematic review support the use of triple therapy but there is inadequate evidence for quadruple or higher combinations
Heterogeneity in the effect estimates seems to result from variable effectiveness of different drug combinations, trial duration, and problems with study quality
Introduction
In 1987 zidovudine was introduced for the treatment of HIV infection. Since then there has been an escalation in the number of antiretroviral agents. Sequentially, treatment with two and then three drugs has become rapidly accepted.1–5 Treatment with four or more drugs has also been proposed. 3 6
Influential clinical guidelines tend to be based on individual selected clinical trials, often published as conference abstracts. 3 4 7 Early results from individual studies can be unrepresentative.8 Support for the clinical benefit of increasing drug combinations comes from well conducted cohort studies,9–14 but the length of follow up is still too short to assess the long term clinical benefit of triple therapy.
Systematic reviews have examined questions about the effectiveness of specific drugs and combinations or have included trials with a mixture of patients who have and have not received drug treatment.15–20 We carried out a systematic review on the effectiveness of increasing numbers of drugs used in combination. To reduce the potential for confounding by established drug resistance we looked only at those patients who had not previously received antiretroviral therapy.
Methods
Search strategy and inclusion criteria
This review was conducted to the suggested QUOROM guidelines standards.21 We looked for randomised controlled trials of antiretroviral therapy in HIV patients (up to the end of February 2001) in Medline, the Cochrane Library, Embase, CINAHL, PsycLIT, Healthstar, appropriate internet sites such as AIDSTRIALS, and citation lists. We also contacted pharmaceutical companies. There was no language restriction. We included studies only if they included patients who were HIV positive (any stage) and were aged ≥12 years with less than six months' previous antiretroviral therapy or if less than 30% of patients had previous therapy or if patients who had never had therapy were reported separately. The accepted interventions were any licensed (United Kingdom or United States) antiretroviral drug (or combination) compared with any other antiretroviral drug or placebo or no treatment. We excluded studies if they lasted less than 12 weeks.
We assessed studies for quality using a standard checklist.22 Data were extracted by two independent reviewers. We included and listed in the review those trials that did not provide any useful measure of variance or had no events, but the data from these trials could not be used in the analyses.
Data analysis
Data were collected on all relevant outcomes, with disease progression and deaths as clinical outcomes and CD4 count and viral load as surrogate markers.
To take account of the large dropout rates but to maximise the length of time in the trial, we measured CD4 count and viral load at the longest time point when at least half of the total number of patients in each arm remained.
Antiretroviral drug comparisons included in analyses of clinical outcomes and surrogate markers
Meta-analysis
For continuous outcomes (CD4 count and viral load change) we calculated the treatment effect for individual trials as the treatment effect (that is, mean change) minus the control effect. We calculated the standard error of the weighted mean difference by adding the variances of the change in outcome in both groups and taking the square root. For triple therapy we also present data on viral load as the proportion of patients in whom concentrations of plasma virus became too low to be detected (<50 copies per ml). We pooled data using the inverse variance method of weighting (for continuous outcomes) and the fixed effects Peto method for event rates.23 Significance was set at P<0.05. We assessed statistical heterogeneity using the χ2 test. 24 25 When there were several arms within a trial that allowed more than one comparison per arm we weighted the number of events and the number of participants so that each participant was used only once.
We explored heterogeneity using sensitivity and subgroup analyses and fixed effects weighted regression techniques (Stata 5.0 software), with the covariates of trial duration, baseline CD4 count/viral load, dropout rates, drug dose, specific drug or drugs (presence of protease inhibitors or zidovudine), change in CD4/viral load (mean/median/change/end point), sensitivity of the viral load assay, and blinding and concealment of allocation.
We assessed publication bias visually using a funnel plot and statistically using Egger's and Begg's tests (Stata 5.0).

Funnel plots of CD4 count results for monotherapy versus placebo, double therapy versus monotherapy, and triple therapy versus double therapy
{kind=link}
Results
Quantity, quality, and characteristics of trials
Out of over 2000 search “hits” we retrieved 700 papers and finally included 90, which referred to 54 different trials26–86 and 20 404 patients. The trials were generally of good quality and randomised. Concealment of allocation was confirmed in a third, most were double blind, and participants in each arm were comparable within trials. Over 80% of the participants were men, with an average age ranging between 27 and 40 years. More patients were asymptomatic than at any other clinical stage, mean baseline CD4 counts ranged from 83-660 cells per μl, and mean viral load ranged from 2.35 to 7.35 log copies per ml. The length of the trials varied from 12 weeks to 4.8 years, although follow up was not always clearly reported.

Effect of zidovudine monotherapy versus placebo on disease progression or death. Figures are number of events/number of participants
{kind=link}

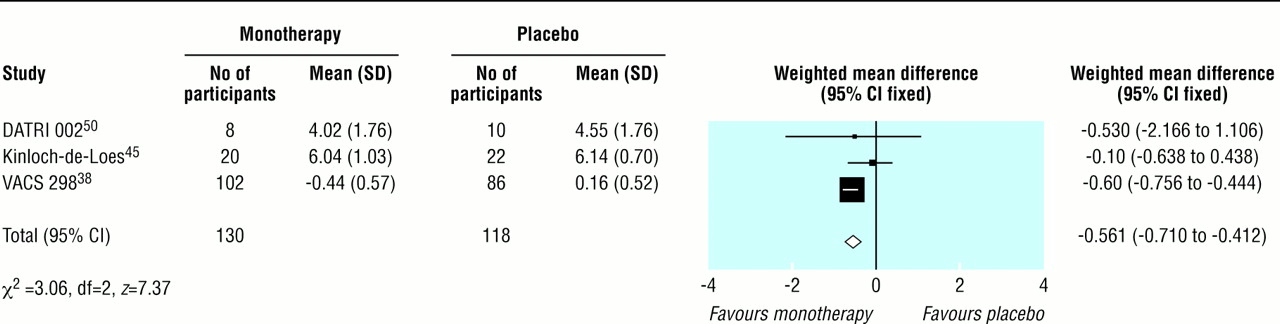
Effect of zidovudine monotherapy versus placebo on change in mean (SD) CD4 count (cells per μl)
{kind=link}
The table lists the comparisons available for the analyses. Zidovudine was the only monotherapy compared with placebo or no treatment. The most common double therapies were two nucleosides, most which were compared against zidovudine or didanosine monotherapy. Triple therapies were mainly based on the currently advised pattern of two nucleosides (usually zidovudine plus didanosine or lamivudine) with the addition of a protease inhibitor or a non-nucleoside. One trial compared quadruple therapy (two nucleosides plus ritonavir plus saquinavir at lower doses given to boost each other rather than as a true full dose quadruple combination) and therefore was not incorporated into the analyses.78 Other unusual interventions (such as cyclical or intermittent therapies) were not included in the analyses. We classified immediate versus deferred zidovudine as zidovudine versus placebo.
Effect of zidovudine monotherapy versus placebo on change in mean (SD) viral load (log copies per ml)
{kind=link}

Duration of trial and odds of disease progression or death with zidovudine monotherapy versus placebo
{kind=link}
Potential publication bias
We found no consistent visual or statistical evidence of publication bias (that is, the tendency that small studies are more likely to be published if they have significant positive results) except for CD4 count for triple versus double therapy, where there was a clear lack of small studies with negative results (fig1). The limitations of the techniques, particularly when there are few trials and there is heterogeneity present, mean we cannot exclude publication bias.

Effect of double therapy versus monotherapy on disease progression or death. Figures are number of events/number of participants
{kind=link}
Main outcomes
Monotherapy compared with placebo
Fifteen trials compared monotherapy with placebo. 26 32–34 36–39 41–45 50 51 Compared with placebo, zidovudine significantly reduced disease progression or death (odds ratio 0.7, 95% confidence interval 0.6 to 0.8), although there was substantial heterogeneity (fig 2). Zidovudine also resulted in an improvement in CD4 count of 47 cells per μl (29 to 65) with no important heterogeneity (fig 3) and a viral load reduction of 0.56 log copies per ml (0.71 to 0.41) with some unexplained heterogeneity (fig 4). The heterogeneity present in the clinical outcome data (range of odds ratio 0.1-1.1, fig 2) was in part explained by the variable duration of the trials: as the trials increased in length zidovudine had a smaller relative effect. At 152 weeks (about three years), as in the Concorde trial,42 the beneficial effect of zidovudine was virtually eliminated (fig 5).
Double therapy compared with monotherapy
We found 14 trials that compared double therapy with monotherapy (fig 6, fig 7, fig 8). 52 53 55–62 66 77 79 80 Double therapy resulted in significantly better clinical outcomes than monotherapy did (fig 6) (odds ratio for disease progression/death was 0.6, 0.5 to 0.7). There was some heterogeneity, but this seemed to be largely accounted for by one large trial of protease inhibitors.79 Sensitivity analysis in which we excluded this trial did not alter the effect size or confidence intervals. In contrast with the results for monotherapy the trial duration did not explain the heterogeneity, despite ranging from six months to three years.

Effect of double therapy versus monotherapy on change in mean (SD) CD4 count (cells per μl)
{kind=link}
Results for surrogate markers were significantly better with double therapy than with monotherapy (fig 7 and fig 8). Subgroup analyses showed that heterogeneity in the CD4 counts was wholly accounted for by the presence of zidovudine or protease inhibitors (fig 7), which suggests that combinations that contain protease inhibitors may be more effective than other double therapies and that monotherapy with zidovudine is less effective compared with other monotherapies. Heterogeneity was present in the analysis of viral load, but exploratory analyses were not informative.

Effect of double therapy versus monotherapy on change in mean (SD) viral load (log copies per ml)
{kind=link}
Triple therapy compared with double therapy
We found 12 trials of triple therapy compared with double therapy (fig 9–fig 12). 68–70 72 73 75 81–86 Triple therapy significantly improved clinical outcomes compared with double therapy (odds ratio for disease progression/death was 0.6, 0.5 to 0.8) (fig 9), although most trials had few events. Only one large trial lasted over a year, and this contributed most events.86 The heterogeneity was attributable to one open label study with few events.73 In a sensitivity analysis that excluded this study we found no change in the estimates of effect size. The results for the surrogate markers (CD4 and viral load) were consistent with those for the clinical outcomes, showing that triple therapy was significantly better than double therapy, though there was substantial heterogeneity in all analyses. Regression analyses of both the CD4 count and the change in viral load indicated that possible causes of this heterogeneity were issues of quality (concealment of allocation and non-blinding) and types of drugs used.

Effect of triple therapy versus double therapy on disease progression or death. Figures are number of events/number of participants
{kind=link}
Other outcomes
Twenty six trials gave information on drug related withdrawals. 30 33 34 36 37 39 42–45 51 55 58 60 61 63 68 69 72 73 75 76 81 82 84 86 Dropout rates were higher with monotherapy than with placebo but no different between double therapy and monotherapy. The results of triple compared with double therapy were heterogeneous. Subgroup classification of trials according to presence of protease inhibitors suggested that there was no significant difference in dropout rates between triple therapy without a protease inhibitor and double therapy without a protease inhibitor. Trials of therapies that contained a protease inhibitor in the triple but not the double arm had significantly higher withdrawals. The exception to this was the PISCES trial,86 the only trial that included saquinavir in the triple arm (fig 13). Only four trials gave useful information regarding quality of life related to health, 27–29 47 71 and they had inconsistent results.

Effect of triple therapy versus double therapy on change in mean (SD) CD4 count (cells per μl)
{kind=link}

Effect of triple therapy versus double therapy on change in mean (SD) viral load (log copies per ml)
{kind=link}

Effect of triple therapy versus double therapy on proportion of participants reaching undetectable viral load. Figures are number of events/number of participants
{kind=link}

Triple therapy versus double therapy and withdrawals due to adverse events related to drug treatment
{kind=link}
Discussion
Principal findings
This systematic review of combination therapy for people with HIV showed a consistently and significantly greater benefit for increasing numbers of drugs up to, and including, triple therapy for clinical outcomes and surrogate markers. Marked variation in the results for many outcomes was greater than could be accounted for by chance alone. When we investigated the effects of potential confounders on the results we found that the heterogeneity for monotherapy was largely explained by decreasing effectiveness over time, which is consistent with the development of drug resistance. For double and triple therapy, the heterogeneity was mainly accounted for by the drugs tested (possible greater effectiveness of protease inhibitors and weaker effect of zidovudine) and issues of quality (blinding and concealment of allocation) for particular trials but was not always consistent between different surrogate and clinical outcomes. We found no published trials on the effectiveness of true full dose quadruple therapy.
Strengths and weaknesses
HIV patients who have never received antiretroviral drugs comprise only a part of clinical practice, but establishment of the effectiveness of such treatment in these patients is fundamental to understanding the overall relative benefit of the drugs, and subsequent treatment decisions are contingent on the initial choice. Though choice of this study population reduced confounding, other potential causes of clinical heterogeneity were reflected in the results. Exploration of heterogeneity with regression techniques suggested that different drugs might explain some of the variation. This conclusion must be tempered with caution as post hoc analyses are purely exploratory and the techniques used are limited, with small numbers of observations. Data on individual patients would allow better exploration of the effect of patient characteristics, although such techniques are usually too expensive and time consuming.87 In addition, some of these findings are based on surrogate end points and should be confirmed by clinical end points, which are less well reported in published trials. Data on adverse events are difficult to interpret in the context of HIV trials in which patient behaviour may differ from clinical practice, and a full evaluation of adverse events should include postmarketing surveillance. Despite a rigorous search for trials, the possibility of publication bias cannot be completely excluded.
Implications and future research
This systematic review provides new evidence that the escalation of combinations of antiretroviral drugs up to triple therapy is an effective strategy. Our results for the relative effectiveness of monotherapy versus placebo and double therapy versus monotherapy are consistent with the results of smaller meta-analyses. 19 20 Also, the overall findings are supported by the results of cohort studies.9–14 However, there is no fully published evidence on the effectiveness of quadruple or higher combinations.
Exploratory analyses of the variation in results showed that differences resulted from the specific drugs used. Both effectiveness and cost considerations indicate that future work to clarify which triple combination is the most effective is as important as investigating the effectiveness of quadruple or higher combinations. As the number of drugs increases, quality of life and safety assume relatively greater importance but are currently inadequately reported.
Better evidence is required. The exploratory analyses of heterogeneity indicate that the design of future trials must be more rigorous and less variable (for example, in trial duration, test drugs, comparators, and clinical stage at entry) and should not rely on surrogate outcomes alone. The research community must respond. There are still important questions to be answered about the effectiveness of existing agents. This may require publicly funded trials which should be carried out within a clear well supported collaborative framework.
Acknowledgments
We thank Jeremy Hawker, Paul Aveyard, Matthias Egger, Sarah Walker, and Abdel Babiker for their valuable comments.
Contributors:RJ was the main reviewer; conducted the search, data extraction, evaluation, and analyses; and wrote the paper. LG performed the double data extraction, advised on direction, and commented on the text. CC advised on and performed the statistics and cowrote the text. CH advised on direction and interpretation of the analyses, made substantial comments on the text, and is guarantor.
Footnotes
-
Funding UK West Midlands NHS Regional Public Health Levy.
-
Competing interests None declared.
References
- 1.↵
- 2.
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.
- 12.
- 13.
- 14.↵
- 15.↵
- 16.
- 17.
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.
- 32.↵
- 33.↵
- 34.↵
- 35.
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.
- 65.
- 66.↵
- 67.
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵