Reported frequency of domestic violence: cross sectional survey of women attending general practice
BMJ 2002; 324 doi: https://doi.org/10.1136/bmj.324.7332.271 (Published 02 February 2002) Cite this as: BMJ 2002;324:271
- Fiona Bradley, lecturer in general practicea,
- Mary Smith, research nurseb,
- Jean Long, lecturer in international health and developmenta,
- Tom O'Dowd, professor of general practice (todowd{at}tcd.ie)a
- a Department of Community Health and General Practice, Trinity College Centre for Health Sciences, Adelaide and Meath Hospital, Tallaght, Dublin 24, Ireland,
- b Health Services Research Centre, Department of Psychology, Royal College of Surgeons in Ireland, Dublin 2, Ireland
- Correspondence to: T O'Dowd
- Accepted 28 November 2001
Abstract
Objectives: To determine exposure to violence by a partner or spouse among women attending general practice and its association with respondents' demographic and personal characteristics; frequency of inquiry about violence by general practitioners; and women's views on routine questioning about domestic violence by general practitioners.
Design: Cross sectional, self administered, anonymous survey.
Setting: 22 volunteer Irish general practices.
Participants: 1871 women attending general practice.
Main outcome measures: Proportion who had experienced domestic violence, severity of such violence, and context in which violence occurred.
Results: Of the 1692 women who had ever had a sexual relationship, 651 (39%, 95% confidence interval 36% to 41%) had experienced violent behaviour by a partner. 78/651 (12%) women reported that their doctor had asked about domestic violence. 298/651 (46%, 42% to 50%) women had been injured, 60 (20%) of whom reported that their doctor had asked about domestic violence. 1304/1692 (77%, 77% to 80%) were in favour of routine inquiry about domestic violence by their usual general practitioner. 1170 women (69%) reported controlling behaviour by their partner and 475 (28%) reported feeling afraid of their previous or current partner. Women who reported domestic violence were 32 times more likely to be afraid of their partner than women who did not report such violence.
Conclusions: Almost two fifths of women had experienced domestic violence but few recalled being asked about it. Most women favoured routine questioning by their practitioner about such violence. Asking women about fear of their partner and controlling behaviour may be a useful way of identifying those who have experienced domestic violence.
What is already known on this topic
What is already known on this topic Domestic violence is associated with physical and psychological ill health
In community surveys, one in four women have experienced such violence
Doctors rarely ask about it, and it is often not recognised even in women with obvious injuries
What this study adds
What this study adds Fear of partner and experiencing controlling behaviour were significantly associated with domestic violence
Anxiety is more strongly associated with domestic violence than depression
77% of all women were in favour of routine questioning about the issue by their usual general practitioner
Introduction
Domestic violence is under-identified and associated with considerable physical and psychological morbidity.1–5 Community surveys indicate that up to one in four women have experienced domestic violence.6–8 In studies in the United States 1 9 10 and Australia,11 between 5% and 20% of the women attending general practice reported experiencing domestic violence in the past year. Less than a fifth of these women had discussed the issue with their doctor.
As there is no universally agreed method of defining and measuring domestic violence, prevalence studies need to collect data reflecting the complexity of this issue.12 Several studies have tried to identify markers of domestic violence for use as indicators during primary care consultations. 1 13 However, although features such as depression, anxiety, and somatisation are associated with domestic violence, they lack predictive value. Some authors have therefore advocated that general practitioners routinely ask all women about domestic violence.14–17 We conducted this study to establish women's reported experience of controlling behaviour, violent incidents, and subsequent injuries; whether general practitioners have asked about domestic violence; and women's views about routine questioning by general practitioners.
Participants and methods
We calculated the sample size to allow us to compare the prevalence of caseness for depression on the hospital anxiety and depression scale between women who had experienced domestic violence and those who had not. We estimated, after reviewing the literature, that 15% of women would have experienced domestic violence and that 10% of the unexposed group would score as depressed. We calculated that a sample size of 790 would have the power (β =80%) to detect a difference of 10% in the prevalence of caseness for depression between exposed and unexposed women with 95% confidence. The clustering of the sample by practice leads to an uncertain design effect of between 1.2 and 1.5. Therefore, we doubled the sample size to 1580. The study was ethically approved by the Irish College of General Practitioners.
In 1996, we invited all 464 general practitioner members of six geographically based faculties of the Irish College of General Practitioners (four urban, two rural) to participate in the study. Thirty four practices agreed to participate, and we chose 22 practices (adequate to recruit the required sample size) to represent maximum diversity in terms of the sex of the general practitioners, singlehanded and group practices, and location. There were 49 general practitioners working in the 22 practices. Between March 1996 and May 1997, each practice collected data for two weeks.
Practice receptionists were asked to hand a patient pack (a consent form with study briefing, a questionnaire for self completion, and a return envelope) to each consecutive female patient over the age of 16 years. The measure of domestic violence included in the questionnaire (see web extra) was adapted from the index developed by Dobash et al and incorporated three dimensions of abuse (controlling behaviours, violent incidents, and consequent injuries).18 Also included were questions on their views about being asked about domestic violence by general practitioners and whether such inquiries had been made; a measure of current level of anxiety and depression (the hospital anxiety and depression scale19); and questions about demographic details. The questionnaire was piloted on 10 women at a Dublin general practice and seven women in a local refuge.
To examine the spectrum of domestic violence, we constructed scales of severity for violent incidents (20 questions) and controlling behaviour (eight questions). For each question, the score ranged from 0 to 3 (never, rarely, sometimes, or often). The violent incident scale thus had a maximum score of 60 and the controlling behaviour scale a maximum score of 24.
We used the Pearson χ2 test to compare proportions in independent groups of categorical data and the χ2 test for trend to identify linear trends. We developed a multiple logistic regression model to identify the independent factors associated with violent incidents.
Results
Reception staff gave questionnaires to 2615 (63%) of the total 4134 eligible women attending the 22 volunteer practices; 1871 (72%) responded. Response rates varied between practices from 38% to 95%, with a median response rate of 79% and a mean of 72%. The number of patients recruited varied depending on the size of the practice (21 to 257). Receptionists reported the following reasons for some women not being asked to take part in the survey: the woman had already been asked to complete the questionnaire; the woman was elderly; or the woman was accompanied by another adult or an ill child.
Of the 1871 women, 1400 (75%) were in a current intimate relationship and 292 (16%) had previously been in one. We excluded the 87 women who had never been in an intimate relationship and the 92 who did not provide data on relationships, leaving 1692 for analysis. Denominators vary because not all respondents answered all questions.
Respondents' were aged 16 to 84 years (median 35 years), and 753 (45%) had a medical card entitling them to free general practitioner care. The card is a good indicator of poverty because it is means tested.
Violent incidents
Six hundred and fifty one women (39%, 95% confidence interval 36% to 41%) had experienced one or more episodes of violent behaviour by a partner (fig 1). Of these, 158 (24%) had experienced one form of violence, 163 (25%) had experienced two or three types of violence, 129 (20%) four to seven types, and 201 (31%) eight or more types. The most commonly experienced behaviours were a partner “punching or kicking the walls or furniture,” “shouting at or threatening the kids,” and having been “pushed, grabbed, or shoved.” More serious violent incidents were also relatively common, with 177/1692 (10%) women reporting having been punched in the face; 168 (10%) punched or kicked on the body, arms, or legs; 154 (9%) choked; and 150 (9%) forced to have sex. Of the 651 women who reported some form of violent behaviour, 298 (46%, 95% confidence interval 42% to 50%) had been injured.

Percentage of women who reported experiencing violence from their partner or former partner (n=1692)
{kind=link}
Controlling behaviour
Figure 2 shows the data on controlling behaviours. The two most common controlling behaviours reported by respondents were being shouted or screamed at (920 women, 54%) and being criticised (832, 49%). After behaviour relating to children was excluded, 1170 women (69%, 95% confidence interval 67% to 71%) reported controlling behaviour by a partner; 569 women (34%) reported one or two of the behaviours, 256 (15%) reported three or four, and 345 women (21%) reported five or more. In addition, 475 women (28%) reported feeling afraid of a current or previous partner.
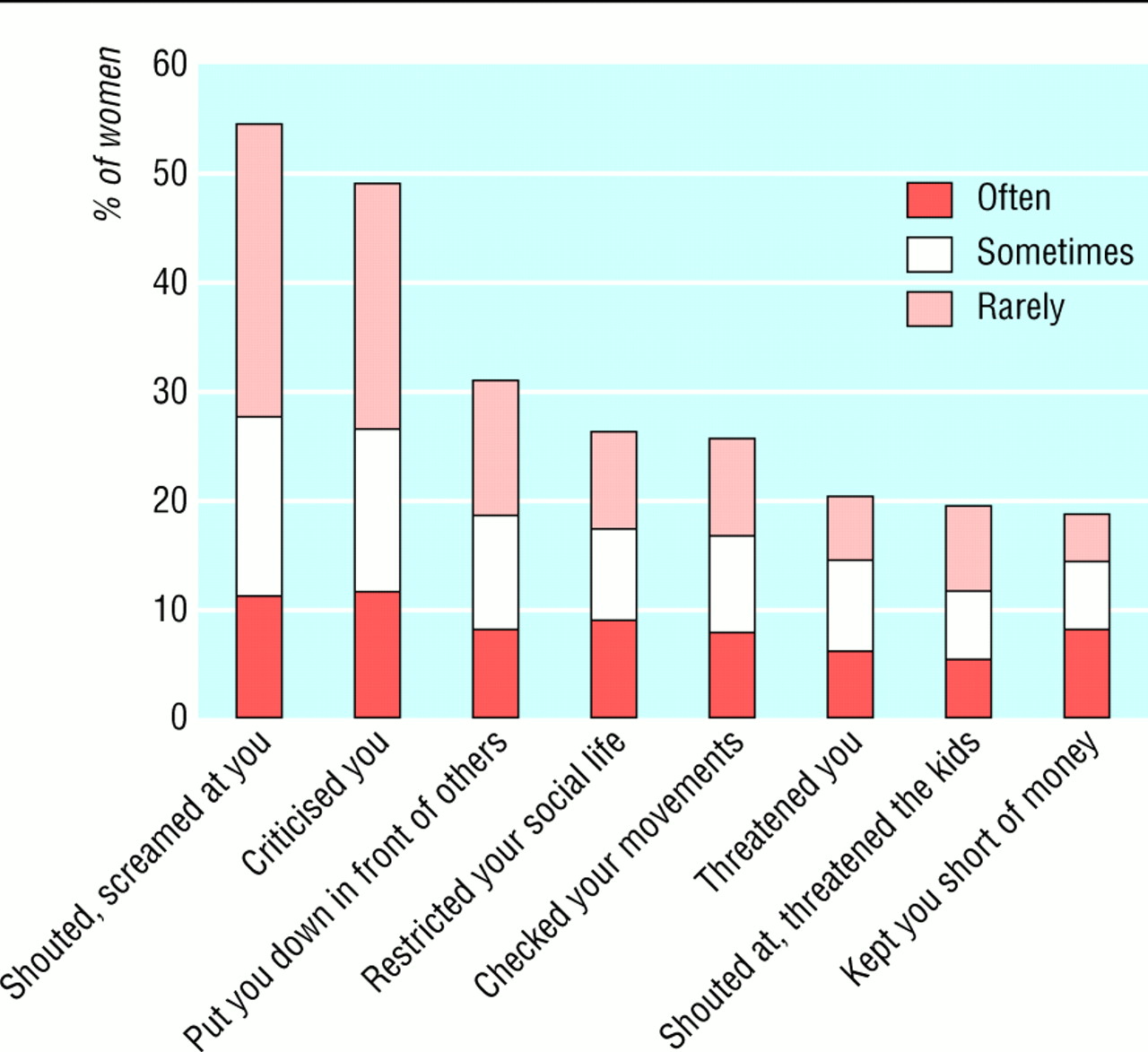
Percentage of women reporting experiencing controlling behaviours by their partner or former partner (n=1692)
{kind=link}
Anxiety and depression
Table 1 shows the hospital anxiety and depression scale scores, according to whether women had experienced violence or injury. The proportions of women who reported ever experiencing violent incidents and injury increased significantly with increasing scores.
Scores on hospital anxiety and depression scale according to experience of violent incidents or injury. Values are numbers (percentages) of respondents with each score
Risk factors
Bivariate analysis with three groups of variables (demographic characteristics, personal characteristics, and contextual factors) indicated that several factors were significantly associated with experiencing violent incidents (table 2). We then constructed logistic regression models to clarify the independent associations between the significant variables and the likelihood of experiencing one or more domestic violence incidents. Table 3 shows the significant factors retained in the final model.
The two contextual factors (afraid of partner and controlling behaviour index score) were strongly associated with experiencing one or more violent incidents by a partner. Women who stated that they were sometimes or often afraid were 32 times more likely to have experienced violence than those who reported that they were never afraid. As controlling behaviour index scores increased, the proportion of women who reported experiencing violent incidents also increased. Women who scored 6-21 were 35 times more likely to have experienced violence than those who had controlling behaviour scores of 0.
Inquiry about domestic violence
Of the 1692 women ever in an intimate relationship, 91 (5%, 95% confidence interval 4% to 7%) reported that their doctor had asked them about a partner threatening them; 1327 (78%, 95% confidence interval 77% to 80%) stated that it would be “all right” for their doctor to ask about violence in relationships and 228 women (13%) were uncertain. Of the 651 women who had experienced one or more violent incidents, 78 (12%) reported that their doctor had asked about a partner threatening them. Five hundred (77%) said that it would be “all right” for their doctor to ask about abuse and 110 (17%) were unsure. Sixty (20%) of the 298 women who had been injured in domestic violence reported that their doctor had asked about a partner threatening them.
Respondents were asked, “If you were coming to the surgery about something else, would you mind if your doctor asked whether you were being threatened, hit, or hurt by your partner or a previous partner?” Only 118 of the 1692 women (7%, 95% confidence interval 6% to 8%) answered that they would mind such routine inquiry by their doctor; 216 (13%) were uncertain.
Discussion
We set out to examine the context and range of domestic violence experienced by women, as well as its frequency. We found a clear relation between experiencing controlling behaviour and violence. The likelihood of experiencing violent behaviour by a partner rose with increasing severity of reported controlling behaviour. There was also a strong association between women reporting fear of their partner and having experienced violence. Women who were sometimes or often afraid were 36 times more likely to have experienced violence than those who were never afraid of their partner. Contextual factors are stronger predictors of violence than demographic or personal factors, and asking the simple question, “are you afraid of your partner?” may be useful.
We found that 39% of women who had ever been in a relationship had experienced domestic violence, which is within the range reported in American and British studies (G Feder, personal communication). 1 9 10 20 The prevalence of domestic violence reported in our survey is double that in Irish community based random surveys,7 which suggests that women who experience domestic violence are over-represented in general practice.
Respondents' experience of violent incidents by demographic characteristics, personal characteristics, and contextual factors
Logistic regression model* to identify factors associated with having experienced one or more violent incidents by a partner
Few women had been asked about domestic violence by their general practitioner. This finding agrees with all other studies in medical settings. Nevertheless, most women stated that it would be acceptable for their usual general practitioner to ask about violence during a consultation about unrelated matters.
We have taken an epidemiological approach to studying domestic violence and are aware that it provides only a partial picture of a complex issue. We used a volunteer rather than a random sample of practices and a systematic sample of women. There may have been some systematic bias in the sampling because women with poor literacy skills were probably under-represented and older women were less likely to be invited to participate. However, overall our findings are likely to be widely applicable to Irish women attending general practice.
Is routine questioning justified?
Routine questioning about domestic violence does not fulfil accepted principles for screening programmes. However, we believe that it is inappropriate to view such questioning as screening. Instead, it should be thought of as a way of uncovering and reframing a hidden stigma. From this perspective, the purpose of questioning is to destigmatise the issue by naming and accepting it, and the perceived need for the doctor to “fix it” is no longer present. This fits with what women who experience violence suggest. Questioning about domestic violence would therefore be justified on this basis.
For general practitioners and doctors in accident and emergency, asking women about fear of their partner and controlling behaviours may be an acceptable and effective way of identifying those who are experiencing domestic violence. Further qualitative research is needed to examine and develop this strategy.
Acknowledgments
We thank the women who completed the study questionnaire and the participating practices, especially the reception staff. We also thank Carol Burns, Deirdre Smith, and Orla Smith for help with field work and data entry; Alan Kelly for statistical advice; and Monica O'Connor and Rebecca Dobash for help with designing the questionnaire.
Contributors: FB wrote the study proposal and received funding. TO'D advised on research design. MS and FB supervised the data collection. FB and TO'D developed the analysis plan. FB carried out the analysis with JL. FB drafted the paper with contributions from all authors. FB and JL wrote the revised version paper with contributions from the other authors. FB and TO'D are guarantors for the paper.
Footnotes
-
Funding Health Research Board in Ireland.
-
Competing interests None declared.
-
 The questionnaire is available as web extra
The questionnaire is available as web extra