Effectiveness of home based support for older people: systematic review and meta-analysisCommentary: When, where, and why do preventive home visits work?
BMJ 2001; 323 doi: https://doi.org/10.1136/bmj.323.7315.719 (Published 29 September 2001) Cite this as: BMJ 2001;323:719
Abstract
Objective: To evaluate the effectiveness of home visiting programmes that offer health promotion and preventive care to older people. Design: Systematic review and meta-analysis of 15 studies of home visiting.
Participants: Older people living at home, including frail older people at risk of adverse outcomes.
Outcome measures: Mortality, admission to hospital, admission to institutional care, functional status, health status.
Results: Home visiting was associated with a significant reduction in mortality. The pooled odds ratio for eight studies that assessed mortality in members of the general elderly population was 0.76 (95% confidence interval 0.64 to 0.89). Five studies of home visiting to frail older people who were at risk of adverse outcomes also showed a significant reduction in mortality (0.72; 0.54 to 0.97). Home visiting was associated with a significant reduction in admissions to long term care in members of the general elderly population (0.65; 0.46 to 0.91). For three studies of home visiting to frail, “at risk” older people, the pooled odds ratio was 0.55 (0.35 to 0.88). Meta-analysis of six studies of home visiting to members of the general elderly population showed no significant reduction in admissions to hospital (odds ratio 0.95; 0.80 to 1.09). Three studies showed no significant effect on health (standardised effect size 0.06; −0.07 to 0.18). Four studies showed no effect on activities of daily living (0.05; −0.07 to 0.17).
Conclusion: Home visits to older people can reduce mortality and admission to long term institutional care.
What is already known on this topic
What is already known on this topic The benefits of regular, preventive home visits to older people are the subject of controversy
A recent systematic review found no clear evidence that preventive home visits were effective
What this study adds
What this study adds This meta-analysis of 15 trials shows that home visiting can reduce mortality and admission to institutional care among older people
Effectiveness of home based support for older people: systematic review and meta-analysis
- Ruth Elkan, research fellow (Ruth.Elkan{at}nottingham.ac.uk)a,
- Denise Kendrick, senior lecturerb,
- Michael Dewey, senior lecturerc,
- Michael Hewitt, evaluation and effectiveness managerd,
- Jane Robinson, professor emeritusa,
- Mitch Blair, senior lecturer in child healthe,
- Deb Williams, lecturera,
- Kathy Brummell, health visitora
- a School of Nursing, Postgraduate Division, University of Nottingham, Queen's Medical Centre, Nottingham NG7 2UH
- b School of Community Health Sciences, Division of General Practice, Floor 13, Tower Building, University Park, Nottingham NG7 2RD
- c School of Community Health Sciences, Trent Institute for Health Services Research, University of Nottingham, Queen's Medical Centre, Nottingham
- d Evaluation Audit Centre for Research, Kingsmill Centre, Sutton in Ashfield, Nottinghamshire NG17 4JL
- e Northwick Park and St Mark's NHS Trust, Harrow, Middlesex HA1 3UJ
- MRC Health Services Research Collaboration, Department of Social Medicine, University of Bristol, Bristol BS8 2PR
- Correspondence to: R Elkan
- Accepted 13 June 2001
Abstract
Objective: To evaluate the effectiveness of home visiting programmes that offer health promotion and preventive care to older people. Design: Systematic review and meta-analysis of 15 studies of home visiting.
Participants: Older people living at home, including frail older people at risk of adverse outcomes.
Outcome measures: Mortality, admission to hospital, admission to institutional care, functional status, health status.
Results: Home visiting was associated with a significant reduction in mortality. The pooled odds ratio for eight studies that assessed mortality in members of the general elderly population was 0.76 (95% confidence interval 0.64 to 0.89). Five studies of home visiting to frail older people who were at risk of adverse outcomes also showed a significant reduction in mortality (0.72; 0.54 to 0.97). Home visiting was associated with a significant reduction in admissions to long term care in members of the general elderly population (0.65; 0.46 to 0.91). For three studies of home visiting to frail, “at risk” older people, the pooled odds ratio was 0.55 (0.35 to 0.88). Meta-analysis of six studies of home visiting to members of the general elderly population showed no significant reduction in admissions to hospital (odds ratio 0.95; 0.80 to 1.09). Three studies showed no significant effect on health (standardised effect size 0.06; −0.07 to 0.18). Four studies showed no effect on activities of daily living (0.05; −0.07 to 0.17).
Conclusion: Home visits to older people can reduce mortality and admission to long term institutional care.
What is already known on this topic
What is already known on this topic The benefits of regular, preventive home visits to older people are the subject of controversy
A recent systematic review found no clear evidence that preventive home visits were effective
What this study adds
What this study adds This meta-analysis of 15 trials shows that home visiting can reduce mortality and admission to institutional care among older people
Introduction
The objective of enabling older people to remain in their own homes has been a cornerstone of government policy for several decades. A recent royal commission on long term care has endorsed this objective, recommending that more emphasis be given to health promotion and other preventive measures as a means of delaying the onset of illness and dependency that eventually lead older people to need long term care.1
One way of promoting health and delivering preventive care to older people is through regular home visiting. Several studies of home visits by teams based in general practices have shown promising results, with home visitors identifying a large number of previously unmet medical and social needs.2-7 Health visitors are well placed to promote the health of older people and to provide surveillance and support. Although British health visitors have historically provided services to mothers and young children rather than older people, the potential of the health visitor in meeting the needs of older people in the community has been widely recognised. 8 9 Despite this, today's generic health visitor devotes little time to older people.10-12
Two previous systematic reviews examined the effectiveness of home visits to older people. In 1993, Stuck et al performed a meta-analysis of 28 controlled trials that evaluated the outcomes of comprehensive geriatric assessment.13 The 28 studies were each allocated to one of five types of assessment, two of which involved home visits to older people. They reviewed nine trials of such visits. 7 14-21 They found significant positive effects of home visiting on mortality, hospital admission and readmission, and nursing home placements.13 A second systematic review of 15 trials of preventive home visits to older people was undertaken more recently by van Haastregt et al.22 This review, unlike that of Stuck et al, did not involve meta-analysis of the 15 trials. 7 14-18 23-30 Van Haastregt et al found no consistent evidence that preventive home visits had a significant effect on any outcome.22
Both these previous reviews have limitations. Stuck et al13 did not include five controlled trials of home visiting to older people, all of which were published at the time they undertook their meta-analysis but which we assume did not meet their inclusion criterion of involving comprehensive geriatric assessment. 24 26 31-33 In the review by van Haastregt et al, the failure to pool the results of the trials was a considerable limitation. The fact that meta-analysis was not performed means that it is possible that significant effects were not detected, and this may in part explain their less positive results.
In view of the shortcomings of previous reviews, and the lack of consistency between their findings, we thought it important to undertake a meta-analysis of all relevant studies available to date to clarify the benefits of preventive home visiting. We report the results of this systematic review and meta-analysis.
Method
As part of a larger systematic review to assess the effects of home visiting to all client groups, including parents and children, we reviewed studies on the effects of home visits to older people (aged 65 years and above). We have presented only those results relating to older people.
Search strategy
We searched Medline for 1966-97, CINAHL for 1982-97, and Embase for 1980-97. We also searched the Cochrane Library and the internet. We hand searched the journal Health Visitor for 1982-97 and scanned reference lists of review articles for relevant literature. We contacted key individuals and organisations to trace unpublished work and placed advertisements in relevant journals to identify unpublished work.
Inclusion criteria
Papers were included in the review if they reported an empirical study, with a comparison group, evaluating a home visiting programme. Randomised and non-randomised controlled trials were included. The home visitor had to undertake tasks within the scope of British health visitors—namely, surveillance, support, health promotion, and the prevention of ill health. The intervention had to involve the pursuit of a wide range of preventive outcomes rather than a single goal such as the prevention of falls or increased uptake of immunisation. We excluded studies in which the home visitor was a specialist in a branch of nursing other than health visiting (for example, community psychiatric nursing or district nursing) and those in which the intervention was delivered solely by volunteers. We also excluded studies that involved only screening and referral, with no other input from the home visitor. We obtained the full text of all studies identified by the search. Disagreements about whether a study met the inclusion criteria were settled through joint discussion of the research team.
We found 1215 references through the searches. Of these, 102 studies fulfilled our inclusion criteria, of which 15 studies reported outcomes relating to older people. 15-17 19 23-35 Nine studies did not meet our inclusion criteria (table 1). 7 14 18 20 29 30 36-38
Excluded studies
Quality rating
We assessed the quality of the studies included in the review by using the Reisch scale,39 which covers the purpose of the study (including prespecification of outcomes and expected effect sizes), experimental design, determination of sample size, description and suitability of treatment/management, masking, subject attrition, and evaluation of participants and treatment/management. The quality of the studies ranged from 0 to 1, with higher scores representing better quality studies. As there is no consensus about the cut off between good and bad studies, the score should be interpreted as indicating relative quality. Three members of the research team scored the papers for quality (DK, MH, MB); they were blind to the name of the publication, authors, results, and conclusions. All three reviewers applied the Reisch scale to 19 of the 102 articles to assess inter-rater reliability. The overall intraclass correlation coefficient was 0.74 (95% confidence interval 0.52 to 0.88).
Combining results
When outcomes were measured on a continuous scale we combined effect sizes using Hedges' method and computed an overall value of g (the standardised effect size).40 For categorical variables we combined odds ratios with the fixed effects Peto method.41
Outcomes included in meta-analyses
The 15 studies measured a wide range of outcomes. We performed a meta-analysis only when three or more studies reporting on the same outcome provided sufficient information for this to be undertaken. This meant that we could not use meta-analysis for psychological health, morale, quality of life, wellbeing, and referral to general practitioners and outside agencies. Several studies that examined the same outcomes that we assessed by meta-analysis did not provide enough information to be included (see table 4). Our review also included two studies that were not randomised. 32 35 Findings from these studies were not entered into a meta-analysis (see table 4).
Meta-regression
In addition to meta-analysis we used meta-regression to see whether the effect sizes that we had extracted could be predicted by study characteristics. We regressed log odds ratios on the predictors, weighted by the inverse of sampling variance.42 We used three characteristics: population (the general population of older people v those at risk of adverse outcomes); duration of the intervention (up to two years v over two years); and age group (<75 v ≥75 years).
Heterogeneity
Although the number of studies that reported any given outcome was small, we calculated formal tests of homogeneity41 (see figure legends). We did not see the use of random effects models as helpful here because the studies we examined were on different groups of participants and used interventions that were far from standardised, and so we believed the solution was to try to explain differences rather than to average what cannot be effectively averaged. We therefore carried out meta-regressions when there were sufficient studies.
Publication bias
We took no formal steps to look for publication bias, such as by plotting effect sizes or by calculating test statistics. In most cases there are few studies on any given effect, and any formal method would have had little power.
Results
Fifteen studies that met our inclusion criteria reported outcomes relating to older people; 13 were randomised controlled trials. 15-17 19 23-34 The two others used a quasi-experimental design. 32 35 The 15 studies were divided into two groups: one group of nine studies assessed members of the general elderly population, 15-17 23 25-31 a second group of six studies assessed vulnerable older people who were at risk of adverse outcomes. 19 24 32-35 The second group consisted of four studies of older people recently discharged from hospital who were at risk of further admissions 19 32-34 and two studies of frail older people who had been referred to home care agencies. 24 35
The aims and content of the studies are shown in table 2. The characteristics of all 15 studies and their quality scores are shown in table 3. Details of the results of the studies are shown in table 4.
Aims, outcome measures, and content of interventions of studies included in review of home based support for older people

Log odds ratios and 95% confidence intervals for mortality in general elderly population (test for homogeneity: Q=6.91, df=7, P=0.44) and frail elderly population (Q=0.87, df=3, P=0.83)
{kind=link}
Findings
Of eight trials that measured mortality in elderly people in general, 15-17 23 26-28 31 three reported significant reductions.15-17 Meta-analysis of these trials gave a pooled odds ratio of 0.76 (95% confidence interval 0.64 to 0.89), indicating that home visiting was associated with reduced mortality. Five studies assessed mortality among frail older people who were at risk of adverse outcomes. The pooled odds ratio of four randomised trials 19 24 33 34 was 0.72 (0.54 to 0.97), again indicating that home visiting had a significant effect (fig 1).
Table 3. Quality scores and characteristics of studies
Outcomes of home visits to elderly people: mortality, admission to hospital, health, functional ability, and long term institutional care
Of six studies that measured admissions to hospital in the general elderly population, 15 16 23 27 28 31 only one reported a significant reduction.15 The pooled odds ratio for all six studies was 0.95 (0.80 to 1.09), suggesting that home visiting did not have a significant effect (fig 2). Three studies examined admission to hospital of frail elderly people who were considered “at risk.” 19 32 35 Meta-analysis was not possible because insufficient information was provided. None found any significant effect. Five studies measured health status among the general elderly population, 16 25-27 31 of which two reported improvements. 16 25 Meta-analysis of the results of three studies 16 27 31 showed no significant effects (standardised effect size 0.06, −0.07 to 0.18). Among the studies that assessed the at risk population, the only study that measured health status33 reported no significant effect (fig 3).

Log odds ratios and 95% confidence intervals for hospital admissions in general elderly population (test for homogeneity: Q=1.42, df=3, P=0.04)
{kind=link}
Seven studies measured functional ability in the general elderly population. 16 17 23 26-28 31 None reported a significant improvement in activities of daily living or other similar measures of functional ability. However, the only two studies that measured instrumental activities of daily living 23 28 both reported significant improvements. Meta-analysis of four studies that measured activities of daily living 23 27 28 31 showed no significant effect (standardised effect size 0.05, −0.07 to 0.17). Of two studies that assessed functional ability among older people considered to be “at risk,” 32 33 neither reported significant improvements (fig 4).
Only one of five studies that reported admission to residential nursing homes of members of the general elderly population 15 16 23 27 28 found a significant reduction.28 However, meta-analysis of the results of four of these studies 15 16 27 28 gave a pooled odds ratio of 0.65 (0.46 to 0.91), indicating that home visiting did have a significant effect in reducing admissions.
Of four studies reporting admission to institutional care of older people considered to be at risk, 19 24 32 34 two reported significant reductions. 19 24 The pooled odds ratio for the three randomised trials entered into a meta-analysis 19 24 34 was 0.55 (0.35 to 0.88), suggesting that home visiting was successful in reducing admissions for at risk older people (fig 5).
Meta-regressions
Our meta-regressions showed that none of our three predictors (population type, duration of intervention, and age group) had any effect on mortality or admissions to institutional care. The analysis of hospital admissions was complicated by the small number of studies, the lack of any studies on elderly people who were considered to be at risk, and the fact that one study31 was of poor methodological quality.
Discussion
Our review of the results of home visiting programmes shows that home visiting is effective in reducing mortality and admission to long term institutional care among members of the general elderly population and frail older people who are at risk of adverse outcomes. We did not find any significant reduction in admissions to hospital. The observed heterogeneity in relation to this outcome (see fig 2) seems to be accounted for largely by the study of Balaban et al,31 which was of poor methodological quality. Balaban et al conceded themselves that they had failed to control successfully for differences in health status between intervention and control participants at entry into the trial, resulting in a control group with better health than the intervention group. The lack of any significant effect in reducing admission to hospital may also have been the result of two opposing effects: on the one hand home visiting may have resulted in increased admissions of older people whose need for hospital care might otherwise have been neglected; on the other hand, some admissions might have been averted through home visits.
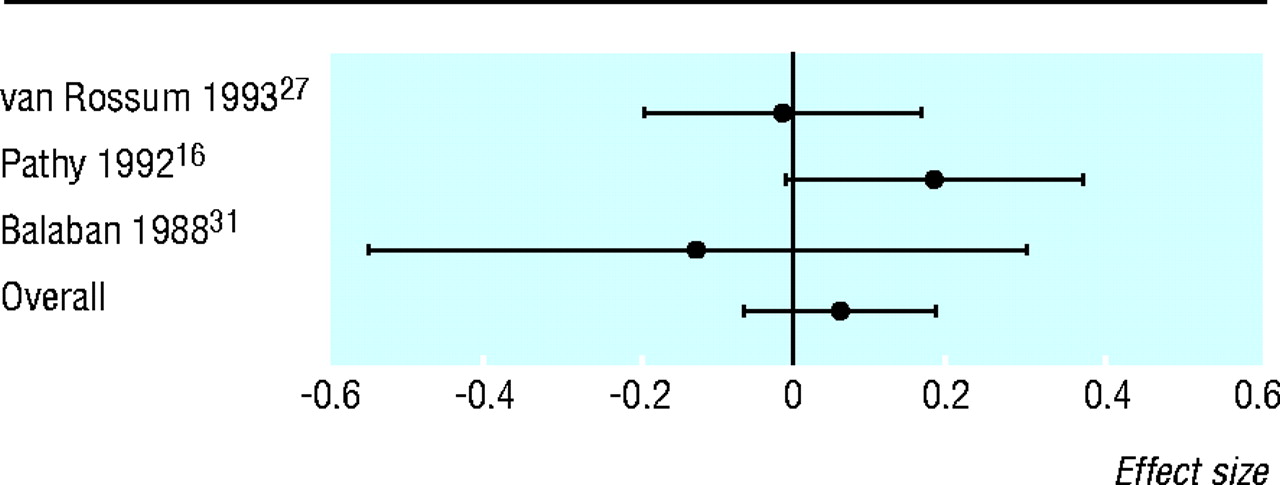
Effect sizes and 95% confidence intervals for health status (test for homogeneity: Q=2.89, df=2, P=0.24)
{kind=link}

Effect sizes and 95% confidence intervals for functional ability (test for homogeneity: Q=3.67, df=3, P=0.30)
{kind=link}

Log odds ratios and 95% confidence intervals for institutional care in general elderly population (test for homogeneity: Q=3.19, df=3, P=0.36) and frail elderly population (Q=2.64, df=2, P=0.27)
{kind=link}
Impact on health and functional status
The absence of evidence of improved health and functional status requires explanation. Undoubtedly one reason for the failure to find any significant differences between intervention and control groups was that those in poorest health had died, so that this outcome could be measured only on a subset of the original sample—namely, those who had survived. Another possible explanation is that where self rated measures have been used, the presence of the home visitor may have encouraged older people to express their problems more easily, thereby obscuring differences between intervention and control group. The tools used may not have been sensitive enough to detect modest improvements in health or functional ability.27 Also, chronic and relatively intractable health and functional problems may require a greater, or different type of, input than that provided by the home visitors in the studies we reviewed.17
Characteristics of home visiting programmes
Why some of the programmes were more successful than others in reducing mortality is puzzling, given that this was not the primary goal of any study. The three studies of members of the general elderly population that reported significant reductions in mortality15-17 did not share any characteristics that differentiate them from the other studies in this group (see table 3). One feature is the breadth of response of the health visitor. In the inner city group in the study by Vetter et al17 and in the study by Hendriksen et al15 the health visitor referred to a wide range of outside agencies, whereas in the rural group in the study by Vetter et al and in other studies that showed no reduction in mortality there was a narrower focus on referral to a general practitioner.
It is difficult to know which components of the home visitors' interventions made a difference to any of the outcomes assessed. As all the programmes were multifaceted, the independent effect of a particular component of care was difficult to assess. Moreover, in the papers we reviewed, descriptions of what the home visitor did were brief, giving little feel for the processes involved. Future studies would benefit from a greater focus on the process of delivering care and on attempting to identify which components of the intervention work.
Our finding from the meta-regression that the effect of home visiting did not depend on whether the intervention was targeted at elderly people who are at risk or whether it was delivered more widely is interesting. It suggests that the exclusion of people who are not at increased risk from such interventions is not, on the present evidence, justified. Similarly, the finding that the effect of home visiting did not depend on the age of participants suggests that the exclusion of “younger” elderly people from such interventions is also unjustified. However, more work is required to test our findings here, as the evidence from individual studies we reviewed suggests that those in poorer health benefit more from the intervention27 and that interventions targeted more intensively on those identified as having problems are more effective.16 A recent study by Stuck et al, published after the end of our literature search, found that disability was reduced in older people at low risk at baseline but not in those at high risk.38 More work is clearly required to assess which populations benefit most from home visiting. Further work could also assess the optimal intensity of home visiting. As several studies did not report the intensity of visits, the importance of this factor was difficult to gauge.
Comparisons with other studies
Our findings are in marked contrast to those of van Haastregt et al,22 who, in the absence of a meta-analysis of the results of the trials they reviewed, failed to find evidence that home visiting resulted in any consistent positive outcomes. Though only four out of the 15 studies we reviewed found a significant effect on mortality, we have shown significant positive effects by combining data. Similarly, only three of the 14 studies showed a significant reduction in admissions to institutional care. 19 24 28 Yet by pooling data from all the studies that assessed this outcome, we showed significant positive effects. It seems that the decision of van Haastregt et al not to perform a meta-analysis might have led them to underestimate the effectiveness of preventive home visits to older people.
Clearly, all meta-analyses contain heterogeneity. However, unlike van Haagstregt et al, we did not consider that differences between the interventions meant their results could not be combined. By grouping our trials into two more homogeneous types of intervention (those aimed at the general elderly population and those aimed at frail older people who were at risk of adverse outcomes), we considered that meta-analysis was justified. While the number of trials in each meta-analysis was small, the results are encouraging, confirming the earlier promising findings of Stuck et al.13 On the basis of our own results, we cannot endorse the conclusion of van Haastregt et al that the evidence of effectiveness is so modest and inconsistent that home visits to older people should be discontinued. On the contrary, we believe that further trials to assess the effectiveness of home based support to older people may confirm our positive findings, and we look forward to the results of ongoing trials.43
Acknowledgments
The views expressed in this paper do not necessarily reflect those of the NHS Executive.
Contributors: JR conceived the idea for the study and initiated and coordinated it. DK, RE, and MD contributed to discussions about core ideas, the design of the study, and the interpretation of the data and wrote the paper. MD undertook the statistical analyses. MH and RE collected the data. DK, MB, and MH carried out the quality scoring. JR, MB, MH, KB, and DW participated in discussions on core ideas, contributed to the study design, and provided critical feedback on the intellectual content of the paper. RE will act as guarantor for the paper.
Footnotes
Editorial by Clark
Funding NHS research and development health technology assessment programme.
Competing interests JR has been reimbursed by the Community Practitioners and Health Visitors Association, the Royal College of Nursing, and the Royal College of Practitioners for attending conferences.
References
Commentary: When, where, and why do preventive home visits work?
- Matthias Egger, senior lecturer in clinical epidemiology. (m.egger{at}bristol.ac.uk)
- a School of Nursing, Postgraduate Division, University of Nottingham, Queen's Medical Centre, Nottingham NG7 2UH
- b School of Community Health Sciences, Division of General Practice, Floor 13, Tower Building, University Park, Nottingham NG7 2RD
- c School of Community Health Sciences, Trent Institute for Health Services Research, University of Nottingham, Queen's Medical Centre, Nottingham
- d Evaluation Audit Centre for Research, Kingsmill Centre, Sutton in Ashfield, Nottinghamshire NG17 4JL
- e Northwick Park and St Mark's NHS Trust, Harrow, Middlesex HA1 3UJ
- MRC Health Services Research Collaboration, Department of Social Medicine, University of Bristol, Bristol BS8 2PR
This is the second of two reviews of trials of preventive home visits to elderly people published in the BMJ in the past 18 months. Elkan et al conclude that home visits reduce mortality and admissions to nursing homes, whereas last year's review found no evidence supporting their effectiveness and argued that existing programmes should be reconsidered.1 Why did the two reviews reach such contrasting conclusions?
The main reason is the different methodological approaches adopted by the two groups. Van Haastregt et al reported the results from individual trials as “no significant effects” or “significant favourable effects.”1 For example, they found a “significant” reduction (P<0.05) in admissions to institutions in only two out of seven trials and that overall effects were “modest and inconsistent.” This “vote counting” approach is clearly unsound as it ignores the direction and size of effects from individual studies and their confidence intervals.2 3 If the BMJ and other journals adopt the recent recommendation that “the description of differences as statistically significant is not acceptable,”4 then the confusion created by such analyses could be avoided.≤0.05)≥
In contrast to the paper by Van Haastregt et al the present review used meta-analysis to summarise results. The potential of this approach is illustrated in the figure, which shows the effects on admission to long term care: six out of eight trials show a beneficial effect of preventive home visits. The evidence against the null hypothesis was fairly strong in two trials (Stuck P=0.021 and Hall P=0.025) but weak in the others (P>0.10). The pooled analysis, however, indicates that there is convincing evidence for a clinically important reduction in the risk of admission to long term institutional care (P=0.001). The reduction in the odds of admission is likely to be at least 17% and could be as large as 51%.

Meta-analysis of eight trials of effect of preventive home visits on admission to long term institutional care. Data taken from table 4. Elkan et al's classification of study population (general elderly population or frail elderly) and mortality in control groups are also shown
{kind=link}
Van Haagstregt et al argued that the data should not be combined statistically, given the heterogeneous nature of the interventions and the populations enrolled in the different trials.1 Interestingly, there was little evidence of heterogeneity between trials in the analysis shown in the figure (P=0.46) and those performed by Elkan et al. The power of tests of heterogeneity is notoriously low and combining studies is always questionable if there is important clinical heterogeneity. However, only by graphically and statistically analysing effect estimates from individual trials can we identify factors introducing heterogeneity. Elkan et al attempted this but their analysis was limited to a few crude factors. For example, they explored the importance of the underlying risk by stratifying trials according to whether older people from the general population or frail elderly people had been enrolled. They found no difference between these groups, which may be due to misclassification of the Hall study. This trial was supposedly performed in frail elderly people, but mortality in the control group was low (see figure). When the effects are ordered according to mortality, as shown, they get smaller with increasing mortality in the control group (figure). This important finding was recently confirmed by Stuck et al in a trial designed to examine effects in older people at low and high risk for admission to a nursing home.5
The analysis carried out by Elkan et al found no improvement in functional status, which is inconsistent with the rationale for home visits. How could mortality and admissions to a nursing home be reduced without an effect on functional status? Unfortunately, only four studies contributed to this analysis, confidence intervals were wide, and Elkan et al did not contact investigators to obtain additional data. Future reviewers should collaborate with original investigators to define the exact characteristics of interventions, obtain data on implementation and adherence, and standardise outcome measures and quality assessment. Several additional trials which have been published recently will increase the power of their analyses. The results are likely to generate useful hypotheses, which should be addressed in trials that are powered to examine effects across prespecified interventions and subgroups of elderly people. Trials and meta-analyses show that preventive home visits can work. The challenge now is to tease out which components of the intervention are effective and which populations are most likely to benefit.
Acknowledgments
I am grateful to Andreas Stuck, John Beck, and Nicola Low for helpful comments.
Footnotes
Competing interests None declared.